


Catarina Gonçalves da Silva Carvalho1; Vanessa da Nóbrega Vilela1; Amanda Eugênia Almeida Rocha1; Gustavo de Sá Menezes Carvalho2; Emmanuel Rodrigues de França3; Aldejane Gurgel de Amorim Rodrigues4
Exogenous Ochronosis is a rare skin disease. It is usually associated with the topical use of hydroquinone, resulting in a grayish or bluish black hyperpigmentation due to dermal deposition of ocher pigment. There is no gold standard treatment and the therapeutic options are generally not effective. We report a case of a patient with exogenous achronosis after use of Hydroquinone, treated with CO2 Laser and showing very good results.
Keywords: HYDROQUINONES; LASER THERAPY; OCHRONOSIS
Exogenous ochronosis is a rare disease characterized by asymptomatic, bluish-black or grayish hyperpigmentation, typically located on the face, however it can involve the neck, dorsum and extensor surfaces. 1.2 It arises more commonly as a side effect of hydroquinone; nevertheless it may be associated with phenol, mercury, or antimalarial drugs or other medicaments. 3 There is microscopic dermal deposition of ocher colored pigment, histologically similar to the congenital endogenous phenomenon known as Alkaptonuria, when there is accumulation of homogentisic acid in the cartilage, cardiac valves and skin. 1.3
The hydroquinone induced hyperpigmentation mechanism remains unclear. 1.2 There are reports of exogenous ochronosis in practically all ethnic groups, even with the use of low concentrations of the substance (2%) and for a short period of time (6 months). Nonetheless, this condition is in fact more frequent in higher phototypes after the prolonged use of hydroquinone in high concentrations. 2.3 Penneys has attributed the skin hyperpigmentation to the inhibition of the homogentisic acid oxidase enzyme by hydroquinone, resulting in homogentisic acid buildup that polymerizes to form the ochronotic pigment. 4
There are three clinical phases: Phase I (presence of erythema and mild pigmentation), Phase II (pigmented papules with caviar-like appearance and atrophy) and Phase III (papulonodular lesions surrounded or not by inflammation). 1.5
Several treatments have been used, however, there are in general high refractoriness rates and poor results. There is a report of an exogenous ochronosis case following the use of hydroquinone that was treated with CO2 laser with quite satisfactory results.
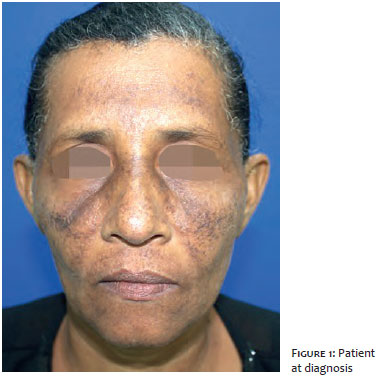
A 46-year-old, Fitzpatrick phototype V patient sought care at the dermatology clinic reporting dark spots on the face (Figure 1). The patient was using a 4% hydroquinone formula for the treatment of melasma for approximately 5 years, with progressive worsening of the lesions. At the initial examination, the patient had poorly delimited papules and hyperchromic macules in the forehead, nasal dorsum and malar regions (Figures 2 and 3), and denied any other symptom or similar family history, altered urine color, hyperpigmentation of the sclera's, underarm's or joint's skin. The patient also denied the oral use of medication and comorbidities.
Treatment with fractional CO2 laser was initiated on the face using the device Dual Deep (Lutronics, Korea). A 120mm tip was used, with the parameters of energy and density set at 120mJ and 150 points per cm2, respectively. The treatment was repeated monthly during 1 year (12 sessions), with significant improvement of the clinical picture (Figures 4 and 5).
The treatment of exogenous ochronosis is deemed as difficult, meaning that prevention is therefore extremely important. The use of hydroquinone in lower concentrations, protection against the sun, early diagnosis of irritation and discontinuation of treatment in the absence of clinical response within 6 months are important preventive measures. 4.6 Avoiding the use of the triggering substance is beneficial, however several years might be required up until some degree of improvement is obtained.
The studied patient has Fitzpatrick's phototype V and has undergone prolonged treatment with hydroquinone – the main risk factors described in the literature.
Several treatments have been used, usually with frustrating outcomes. Treatment with trichloroacetic acid and cryotherapy are not effective. 7 In some cases tretinoin can improve lesions, however it may sometimes lead to transient hyperpigmentation. 4.7 Low strength corticosteroids associated with photoprotection showed good results. 7 Satisfactory results were also described with dermabrasion, CO2 laser, glycolic acid peels and Q-switched lasers (694nm ruby and 755nm alexandrite). However, the outcomes are not homogeneous.6.7
The use of CO2 laser for the treatment of exogenous ochronosis is scarcely described in the literature, mainly as an isolated therapy. Diven et al. employed a combination of dermabrasion and ablative CO2 laser with satisfactory outcomes in the periorbital and nasal regions and partial improvement of cutaneous lesion, in a woman high Fitzpatrick phototype 7.8
Exogenous ochronosis is a difficult to treat pathology, with several reports of ineffective therapies in the literature. 5.7 The studied patient had an excellent response to sessions of fractionated CO2 laser, leading to the conclusion that it can be an effective option in some cases of refractoriness.
1. Kindem S, Serra-Guillén C, Guillén C. Hiperpigmentación facial parcheada. Actas dermosifiliograficas 2015;106(4):317-8.
2. Martins VMR, Sousa AR, Portela NC, Tigre CA, Gonçalves LM, Castro Filho RJ. Exogenous ochronosis: case report and literature review. An Bras Dermatol 2012;87(4):633-6.
3. García García, C. Lesiones de la pigmentación cutânea. Medicine - Programa de Formación Médica Continuada acreditado. 2010;10(48):3195-3203.
4. O'Donoghue MN, Lynfield YL, Derbes V. Ochronosis due to hydroquinone. J Am Acad Dermatol. 1983;8(1):123.
5. França ER, Paiva V, Toscano LPN, Nunes GJB, Rodrigues TFA. Ocronose exógena: relato de caso. Surg Cosmet Dermatol. 2010;2(4):319-21.
6. Ribas J, Schettini APM, Cavalcante MSM. Ocronose exógena induzida por hidroquinona: relato de quatro casos. An. Bras. Dermatol 2010;85(5):699-703.
7. Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30(4 Pt 1):555-8.
8. Diven DG, Smith EB, Pupo RA, Lee M. Hydroquinone-induced localized exogenous ochronosis treated with dermabrasion and CO2 laser. J Dermatol Surg Oncol.1990; 16(11):1018-22.
This study was performed at Universitário Oswaldo Cruz – Universidade de Pernambuco (UPE) – Recife (PE), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}