


Guillermo Loda1; Francine Papaiordanou2; Joaquim José Teixeira de Mesquita Filho3; Bruna Souza Félix Bravo4; Luciana de Abreu5; Tullia Cuzzi6
Injectable fillers have long been used for cosmetic purposes and in HIV induced lipodystrophy patients. A foreign body granuloma may be a side effect of the application of absorbable products/temporary and most often the nonabsorbable/permanent fillers. It is not possible to predict the formation of these granulomas, and it may occur regardless of the application technique. In this article we describe the surgical treatment of a patient with multiple granulomas caused by intradermal injection of PMMA in the face, with poor response to conservative treatments, and severe psychosocial impairment due to this unsightly and disfiguring complication.
Keywords: POLYMETHYL METHACRYLATE; GRANULOMA; AMBULATORY SURGICAL PROCEDURES
In the few last years, filling substances have been widely used in aesthetic procedures and for the correction of lipodystrophy in HIV-positive patients. Products containing hyaluronic acid in different densities, bovine collagen, autologous fat, liquid silicone, poly-l-lactic acid and polymethyl methacrylate (PMMA), among others are widely used for this purpose. 1 According to the product's bioavailability and its chemical composition and degradation capacity, these substances can be classified as temporary or permanent, organic or inorganic and autologous or heterologous. 2,3
In order for a substance to be considered safe, some important aspects should be taken into account: it must be biocompatible, phagocytosis resistant, stable, non-migratory, induce the least possible inflammatory response, not be carcinogenic or teratogenic 2.
Polymethyl methacrylate (PMMA) is a polymer composed of synthetic microspheres of 30µm to 40µm, with homogenous surface, conveyed suspended in a 1:3 solution (3.5% bovine collagen and lidocaine) or in carboxymethylcellulose colloid solution. 4 It should be strictly applied in the deeper layers of the dermis. 1,5 It initially promotes volumization, however has the capacity to stimulate neocollagenesis, with long-term effects.
The application of PMMA might be related to some adverse effects, such as nodules, inflammation, allergic reactions, dyschromias, necrosis, infection and foreign body granuloma formation. 6-8. Although described in the literature as rare, these complications are often permanent and very difficult to treat.
The foreign body granuloma can be secondary to absorbable/temporary products and, more often, to nonabsorbable/permanent fillers. It is not possible to foresee the formation of these granulomas, which can occur regardless of the used technique. Granulomas often form many years after the first application. 9
The present paper describes the surgical treatment of a patient bearing multiple granulomas caused by a previous PMMA based intradermal filling in the face, with a poor response to conservative treatments and severe psychosocial compromise due to this unsightly and deforming complication.
A 63-year-old female patient reported having undergone facial filling 18 years before, observing the onset of palpable hardened cylindriform nodular lesions painful on palpation, located in the sites of prior application of the product. The nodules were not adhered to deep subcutaneous planes.
Ultrasonographic examination of the face showed heterogeneous elongated hypoechoic images, superficial and with defined limits, located between the skin and the subcutaneous tissue, bilaterally dispersed in the malar, periorbital, temporal and supralabial regions, in addition to the nasogenian sulcus. Dimensions varied from 3.2 x 0.8 x0.5cm in the left malar region to 3.6 x 2.4 x 0.5cm in the right malar region. Doppler examination evidenced avascular images. A new ultrasound examination was performed 1 year after the first, revealing poorly-defined nodular images with the following measures: 12mm in the left nasal region; 6.6mm in the left nasogenian sulcus; 8.1mm in the superior right labial region; 11.2mm in the right nasogenian sulcus; 14.0mm in the right temporal region; and 11.0mm in the left temporal region. The examinations were performed in diverse laboratories – note that the lesions were first measured in cm and then in mm.
Magnetic resonance imaging of the face (performed with contrast) showed multiple heterogeneous nodular formations, with lobular borders and isointense signal at t1 and predominantly intense in t2 and stir, showing slight contrast uptake, with confluent appearance in the subcutaneous of the malar and mandibular regions, nasogenian sulcus, bilaterally periorbicular, possibly corresponding to foreign bodies.
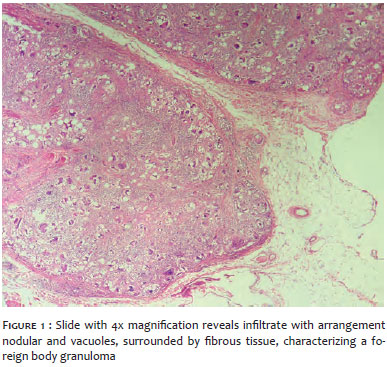
The histology of one of the lesions demonstrated it was a foreign body granuloma (Figure 1).
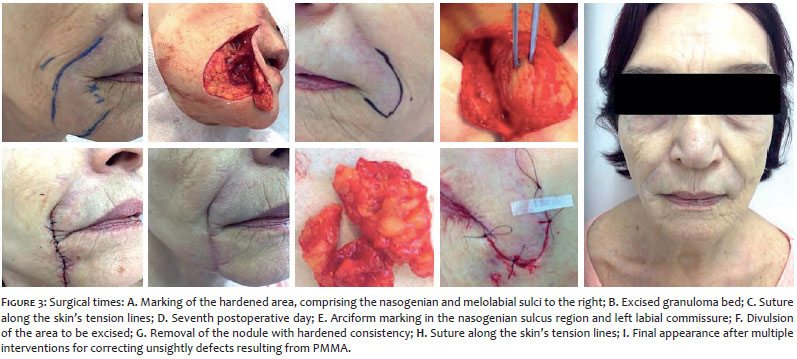
The patient underwent multiple facial surgeries aimed at correcting the unsightly defects secondary to PMMA filling.
Due to the fact that the zygomatic region's surfaces are convex and have multiple static rhytids, a decision was made to perform the w-plasty technique, aimed at obtaining a scar with a more irregular pattern, aligned with the skin's tension lines, thus being less apparent. The w-plasty consists of triangular advancement flaps uniformly interposed, parallel to the relaxed skin tension lines (RSTL). A scalpel blade n. 11 was used, observing a minimum of 60 degrees for the triangles' angles. The closure was performed with simple stitches and nylon thread 6.0.
The nasogenian and melomentonian grooves had lesions with clinical and histological characteristics similar to those in the zygomatic region.
A choice was made to perform long incisions positioned inside the grooves so that they could be hidden in the RSTL.
A "hockey stick" incision was used in the angle of the mouth's region, allowing a more cautious divulsion of the nodules located in that area.
Surgeries with the same characteristics were performed in four surgical times, with intervals of approximately 1 month, progressing with good cicatrization, without infectious complications and satisfactory aesthetic outcome, according to the patient's report (Figures 2 and 3).
Applications of synthetic polymers in the skin generate some degree of inflammatory response, due to either the trauma caused by the application or the interaction of the receptor's tissue with the implant.
The particulate filler's biocompatibility varies according to the particles' size, shape and surface. When they are irregular, they cause greater inflammatory response, while varied sizes induce a higher degree of foreign body reaction. According to the recent literature, granuloma formation occurs in between 0.01% and 2.5% of applications. 2
Three days after the PMMA injection, monocytes invade the implant, and on the sixth day they differentiate into fibroblasts. In two or three weeks the connective tissue infiltrates the material, forming clusters of the product, and the neovascularization becomes more evident. The autologous collagen fibers' density increases during the four months after the application, when the fibrosis and active vascularization. 2
The presence of foreign body giant cells is evident after the first week after the application, reaching its maximum number around the third week and remaining at that level for two months. The late mass development of giant cells indicates the formation of foreign body granuloma formed by multinucleated giant cells and macrophages arranged in palisade with a lymphocytic halo. 1
The reason that the host reacts with a granulomatous inflammatory response in these cases is still unknown. Some authors believe that a mild chronic inflammation may occur due to improper location of the filler or even to the displacement of the material to more superficial skin layers. There are some therapeutic options for the management of this complication: intralesional corticosteroids injections, corticosteroid therapy and oral antibiotics, in addition to allopurinol. In cases that are more severe or resistant to other therapies, surgical excision is mandatory. 1, 2, 5
Several treatments, such as oral and intralesional corticosteroids were tried in the reported case, however with absence of satisfactory response. In addition, the patient described constant pain and dissatisfaction with the lesions' aesthetic appearance. For that reason surgery was proposed to remove the greatest possible number of the most evident granulomas.
The aesthetic result of the removal of granulomas was very satisfactory, since it progressed without unsightly scars, significantly improving the nodular appearance of the analyzed regions, with a high degree of patient satisfaction. The patient continues under ambulatory follow-up, and therapy with allopurinol has been initiated to reduce small residual granulomas. 4
There is not a filling substance that can be deemed as ideal since all materials can cause early or late adverse effects. Although PMMA is relatively safe, the host's immunology is primarily responsible for the different reactions that might arise.
It is crucial that the patient be informed beforehand of the possible complications in advance of undergoing any procedure.
Currently, the trend points towards a choice for absorbable fillers, which have a lower incidence of adverse reactions and do not lead to permanent outcomes.
1. Reisberger EM, Landthaler M, Wiest L, Schröder J, Stolz W. Foreign Body Granulomas Caused by Polymethylmethacrylate Microspheres: Successful Treatment With Allopurinol. Arch Dermatol. 2003;139(1):17-20.
2. Campos DLP, Proto RS, Santos DC, Ruiz RO, Brancaccio N, Gonella HA. Avaliação histopatológica do polimetilmetacrilato em ratos ao longo de um ano. Rev Bras Cir Plast. 2011;26(2):189-193.
3. Thaler MP. Foreign body granulomas caused by polymethylmethacrylate microspheres: an added perspective. Arch Dermatol. 2003;139(11):1505-6.
4. de Barros Silveira LK, de Oliveira FL, Alves T de B, Rambaldi ML, de Andrade FC, Kelmer S de C, Barbosa FC. The therapeutic benefit of allopurinol in the treatment of foreign body granulomas caused by polymethylmethacrylate microspheres. Case Rep Dermatol Med. 2012; 2012: 1-3.
5. Ledon JA, Savas JA, Yang S, Franca K, Camacho I, Nouri K. Inflammatory Nodules Following Soft Tissue Filler Use: A Review of Causative Agents, Pathology and Treatment Options. Am J Clin Dermatol. 2013;14(5):401-411.
6. Park TH, Seo SW, Kim JK, Chang CH. Clinical experience with polymethylmethacrylate microsphere filler complications. Aesthetic Plast Surg. 2012;36(2):421-6.
7. da Costa Miguel MC, Nonaka CF, dos Santos JN, Germano AR, de Souza LB. Oral foreign body granuloma: unusual presentation of a rare adverse reaction to permanent injectable cosmetic filler. Int J Oral Maxillofac Surg. 2009;38(4):385-7.
8. Salles AG, Lotierzo PH, Gemperli R, Besteiro JM, Ishida LC, Gimenez RP, et al. Complications after polymethylmethacrylate injections: report of 32 cases. Plast Reconstr Surg. 2008;121(5):1811-20.
9. Rongioletti F. Granulomatous reactions from aesthetic dermal micro-implants. Ann Dermatol Venereol. 2008;135(1 Pt 2):1S59-65.
This study was performed at the Instituto de Dermatologia Prof. Rubem David Azulay – Santa Casa de Misericórdia do Rio de Janeiro – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}