


Maria Victória Quaresma1; Luciana de Abreu2; Lara Braga Oliveira3; Bárbara Poggi4; Thalyta Valle de Rezende5; Bruna Souza Felix Bravo6
Adverse reactions associated with drugs presenting cutaneous manifestations are among the most common, expressing itself with multiple clinical aspects and causing significant morbidity. The fixed drug eruption (FDE) is a common adverse reaction with cutaneous involvement and is associated with the use of numerous drugs. Dipyrone is a drug with analgesic and antipyretic effects prescribed widely used in Brazil, however, it is known for its potential to triggering adverse reactions, including the FDE. This report shows an EMF case related to the use of dipyrone, with unique clinical presentation and correlate the clinical, histopathological and dermatoscopic found.
Keywords: DERMOSCOPY; FACE; PATHOLOGY
Adverse reactions to drugs can be defined as any response elicited by a given drug that is harmful, unintentional and occurs at the doses used by individuals for prophylaxis, diagnosis and treatment of diseases. 1 Reactions involving the skin, known as pharmacodermy, are among the most common and can have many clinical appearances – from solitary lesions up until generalized pictures. 2 Fixed drug eruption (FDE) is a common pharmacodermy and can be associated with the use of countless medicaments. 3 It was first described by Brocq,1 FDE clinically arises as a macular, erythematous-violaceous, oval lesion with recurrence in previously affected sites, triggered by the re-exposure to the involved drug. This eruption may occur in any body area, mainly affecting mucosal surfaces. 4, 5
Dipyrone is a non-steroidal anti-inflammatory derived from pyrazolone, being widely used as an analgesic. Numerous adverse reactions secondary to dipyrone are known: interstitial nephritis, hepatitis, pneumonitis and severe skin drug eruptions, such as the Stevens-Johnson and Lyell syndromes. 2 Despite being known, the association of this drug with FDE has only occasionally been reported in the literature, often linked to lesions involving the trunk and extremities. 5, 6
In light of these facts, the authors of the present paper report a FDE case triggered by dipyrone, a drug that is widely used in Brazil, however with few reports describing this association. In addition, the unique clinical appearance of the case stands out, with facial involvement (periorbital and nasal regions), correlating it with the relevant histological and dermoscopic findings.
A 30 year-old female patient originary from the Brazilian Southeast state of Rio de Janeiro, bore hyperchromic macules on the face for one month. The patient referred using dipyrone to treat a headache 7 hours before the cutaneous picture emerged. She denied any systemic symptomatology, comorbidities or local trauma. The dermatological examination evidenced hyperchromic, grayish-brown, oval in shape, well delimited macules, bilaterally symmetric in the periorbital regions (Figure 1). There were no lesions in other cutaneous or mucosal sites. The possibility of FDE associated with dipyrone was raised, and the patient was instructed to avoid using this drug.
Four months after the initial event, the patient had recurrence of the picture with the extension of the lesions up until the nasal dorsum (Figure 2). During the examination, she denied the use of dipyrone, however describing the use of a diverse medication that reportedly contained dipyrone in it formulation.
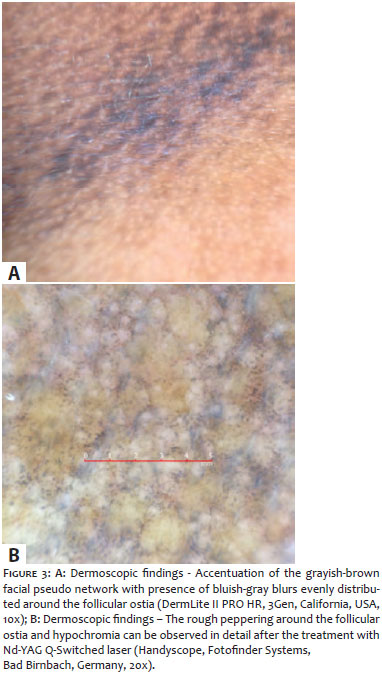
The dermoscopic examination of the bilateral periorbital lesion showed a granular annular pattern with pigmented blurs and multiple bluish-gray dots ("peppering"), evenly distributed around the follicular ostia, with accentuation of the grayish-brown facial pseudo network (Figure 3).
The biopsy of the skin with the lesion was assisted by the dermoscopic examination, being performed where there was greater concentration of the blue-grayish granularity, known as peppering. 7
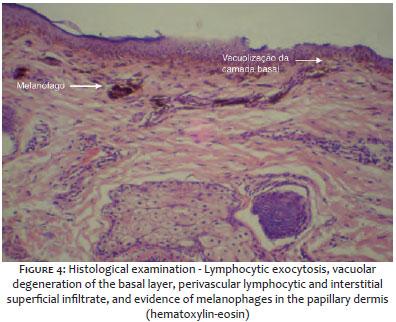
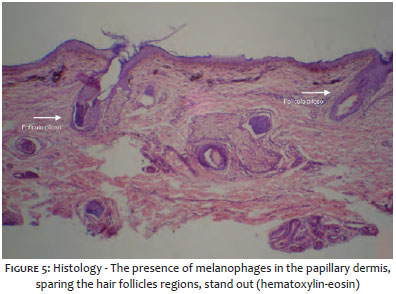
The histological examination revealed: lymphocytic exocytosis, vacuolar degeneration of the basal layer, perivascular and superficial interstitial lymphocytic infiltrate, and melanophages in the papillary dermis, corroborating the diagnosis of FDE (Figure 4). In addition, melanophages were regularly distributed in the superficial dermis among the hair follicles (Figure 5).
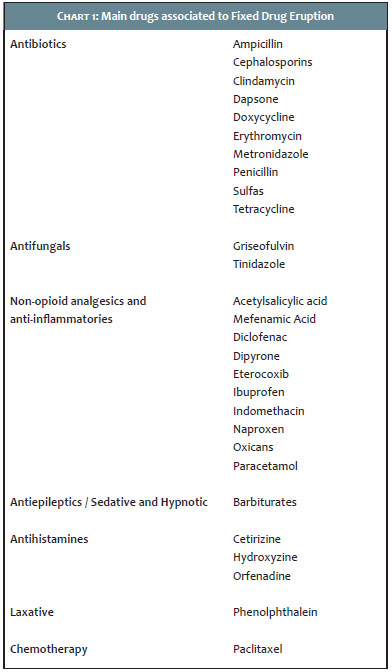
Fixed drug eruption is a drug-related reaction linked to the use of numerous drugs (Table 1), 3-5,8,9 with no gender prevalence, predominantly occurring in the third decade of life. 3,4 Patients with family history of drug allergy or atopy have increased susceptibility to develop this pharmacodermy. 3
The picture usually arises between 30 minutes and 8 hours after the use of the medication; however, manifestations within 24 hours have already been described. Classically, it has the appearance of a single erythematous or violaceous-erythematous, oval-shaped, well demarcated macula, with up to 10cm in diameter, which may progress with residual hyperpigmentation. It rarely emerges with multiple lesions. The more frequently involved regions are the mucous membranes and, in special, the genital and lip regions. 4
The association of dipyrone with FDE is recognized by the literature, however there are few reports describing this relationship. 2,6 According to Sharma et al., 8 FDE triggered by this drug arises as a single lesion, affecting mainly the trunk and extremities. 5,6
In the histological evaluation, FDE in its initial phase shows hydropic degeneration of the basal layer's cells, with apoptotic keratinocytes, lymphocytic perivascular infiltrate in the superior dermis, and may show sparse neutrophils, eosinophils and edema in the superficial dermis. 9 In its late stage, the presence of melanophages in the papillary dermis is remarkable – which can be the only finding in lesions with long development. 5,9
Dermoscopy is an auxiliary diagnosis method that has been standing out for its practicality and clinical applicability, due to its ability to recognize specific standards and criteria established for various dermatoses. The dermoscopic examination has peculiar patterns when performed on the face, since the epidermis presents attenuation and flattening of interpapillary cones and abundance of cutaneous adnexa, such as hair follicles' and eccrine glands' ostia. However, in the adult face, the conventional pigmented network usually seen at dermoscopy cannot be observed, for the epidermal crests are flat or absent; in the face, therefore, the pigmentation is described as a pseudo network, being characterized by brown pigmentation interspersed with circular spaces represented by follicular openings and glandular orifices. 10
In the present case, dermoscopy evidenced a granular annular pattern, with bluish-gray blurs and dots (peppering), predominantly around the follicular ostia, corresponding to the melanophages aggregates in the papillary dermis observed in the histology. The pattern's bluish-gray color is attributed to the depth and extension of the melanin deposit in the papillary dermis. These melanin deposits are the result of the vacuolization of the epidermal basal layer associated with an inflammatory process, with the subsequent "fall" of the melanin pigment into the papillary dermis and phagocytosis by macrophages (melanophages). 7,10
The case's dermoscopic characteristics suggest it is an underlying inflammatory condition. 7 On the other hand, the asymmetric pigmentation, when more pronounced at the edges of the follicular openings, with progressive obliteration of the ostia, is a criterion for suspicion in favor of melanocytic malignant lesions, such as lentigo maligna melanoma type. 10
As a conclusion, recognizing the drug causing the FDE allows the proper management of the treatment, avoiding recurrences. The association of this disease with dipyrone is sparsely reported, especially when linked to the emergence of facial lesions. The use of dermoscopy allows the recognition of typical patterns, such as the observation of the granular, rough peppering as the preponderant dermoscopic criterion in the present case. The pigmentation's symmetrical and regular distribution was key to the suspicion of inflammatory dermatosis, since in most cases this finding corresponds to intradermal melanophages. 7 In this manner, despite the fact that histological analysis is considered the gold standard method for the diagnosis of FDE, in the present case dermoscopy was effective in assisting in the choice of an ideal site for performing the cutaneous biopsy.
1. Brocq L. Eruption erythemato-pigmentee fixe due a l'antipyrine. Ann Dermatol Venereol. 1894;5:308-313.
2. Bentur Y, Cohen O. Dipyrone overdose. J Toxicol Clin Toxicol. 2004;42(3):261-5.
3. Mahboob A, Haroon TS. Drugs causing fixed eruptions: a study of 450 cases. Int J Dermatol. 1998;37(11):833-8.
4. Heng YK, Yew YW, Lim DS, Lim YL. An update of fixed drug eruptions in Singapore. J Eur Acad Dermatol Venereol. 2015;29(8):1539-44.
5. Justiniano H, Berlingeri-Ramos AC, Sánchez JL. Pattern analysis of drug-induced skin diseases. Am J Dermatopathol. 2008;30(4):352-69.
6. Ozkaya-Bayazit E. Specific site involvement in fixed drug eruption. J Am Acad Dermatol. 2003;49(6):1003-7.
7. Bugatti L, Filosa G. Dermoscopy of lichen planus-like keratosis: a model of inflammatory regression. J Eur Acad Dermatol Venereol. 2007;21(10):1392-7.
8. Sharma VK, Dhar S, Gill AN. Drug related involvement of specific sites in fixed eruptions: a statistical evaluation. J Dermatol. 1996; 23(8):530-4.
9. Joshi R. Interface dermatitis. Indian J Dermatol Venereol Leprol. 2013;79(3):349-59.
10. Stolz W, Schiffner R, Burgdorf WH. Dermatoscopy for facial pigmented skin lesions. Clin Dermatol. 2002;20(3):276-8.
This study was performed at the Instituto de Dermatologia Professor Rubem David Azulay - Santa Casa da Misericórdia do Rio de Janeiro – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}