


Camila Carneiro Marques1; Denise Steiner2; Gabriela Momente Miquelin1; Mariana Morais Tavares Colferai1; Eduardo Figueiredo Gatti1
Introduction: Male androgenetic alopecia, has high prevalence and causes great discomfort in patients. The platelet-rich plasma generates an environment acts to create a suitable microenvironment for tissue repair and possibly prolongs the anagen phase of the hair follicles.
Objective: To evaluate the safety, efficacy and viability of the PRP use for the treatment of male androgenetic alopecia. Methods: We selected 08 male patients with androgenetic alopecia. Participants had the side of the scalp randomized scalp to receive PRP or placebo. 3 were performed monthly applications.
Results: Patients who received treatment realized some degree of improvement especially as regards the fall. The results were obtained through the analysis dermatoscopic was evaluated as "trichoscale". We observed an increase of anagen hairs, down telogen hairs and vellus wires and increase terminal wires. The results were statistically significant as the reduction of vellus wires and increase of terminals wires.
Conclusions: This study showed a clinical improvement observed for photos as well as positive results documented by analysis "trichoscale". There was statistical significance of data obtained especially after the first month of treatment.
Keywords: ALOPECIA; PLATELET-RICH PLASMA; MEN
Male androgenetic alopecia is the most prevalent form of alopecia, and although it is socially accepted, it generates great discomfort, low self-esteem and social problems in many of the affected individuals.
In this form of alopecia, the following changes can be observed: alterations in the hair cycle, with miniaturization of follicles, which become thinner and less pigmented (similarly to the vellus), shortened anagen phase, and a greater number of follicles that remain in the chenogen phase, when the follicle is empty.
Its pathogenesis is multifactorial and involves hormonal and genetic factors. In men, the most active androgen is the testosterone, which is converted into dihydrotestosterone by the 5-alpha-reductase type II's action in the dermal papilla, anatomically close to the hair follicle. Dihydrotestosterone has greater affinity to androgenic receptors than to testosterone. Men bearing androgenetic alopecia have higher levels of 5-alpha-reductase in the frontal region as compared to the occipital region. Most of the patients present normal serum androgen levels, meaning that the hormonal mechanism in androgenetic alopecia can be explained by a possible increase in androgens production in the pilosebaceous unit, or by an overexpression or hyperresponsiveness of the androgens' receptors.
Family history is usually positive in male androgenetic alopecia, and there is also a strong genetic association, probably due to polygenic inheritance.
Treatment options for androgenetic alopecia are very limited and include topical application of minoxidil and oral finasteride (FDA approved), isolatedly or in combination. However, there are several secondary side effects have been described, such as headache and increase in other body hairs (with minoxidil), and loss of libido (with oral finasteride).
Platelet-rich plasma (PRP) is produced from processed autologous blood, from which a concentrate of platelets, rich in growth factors (released by the platelets) is obtained. The use of PRP has shown positive effects in the fields of plastic, orthopedic and cardiac surgery, due to its potential tissue repair effect.
The presence of some leukocytes in PRP leads to a natural resistance to infectious processes, reducing the risk of infections in the site to be treated. Platelets are the essential components of this concentrate for they are able to release important growth factors that are important for the tissular cicatricial modulation. The platelets' alpha granules release a number of growth factors, which act by binding to cellular receptors that transmit the signal to the interior of the cells. Platelet-derived growth factor (PDGF) was one of the first factors to be identified. The platelets' PDGF begins the repairing process, stimulating the synthesis of DNA, the chemotaxis and collagen synthesis, processes that are crucial for the wound repair. The transforming growth factors beta (TGF-b) are a group of local mediators that regulate the proliferation and functions of most of the body's cells. Growth factors also activate the proliferative phase and differentiation of the ciliated cells and hair follicular stem cells, producing new follicular units. It has been reported that activated PRP stimulates the proliferation of cells in human dermal papillary layer, increasing the hair follicle cells' survival through its anti-apoptotic effects, and possibly stimulating hair growth, prolonging the anagen phase. 1,2,3
The objective of the present study was to evaluate the safety, effectiveness and viability of using PRP for the treatment of male androgenetic alopecia.
A randomized, placebo-controlled blinded trial was carried out.
Eight male patients with androgenetic alopecia were selected. All met the following inclusion criteria: 18-45 year-old men, clinical diagnosis of androgenetic alopecia, and absence of previous treatment – including the use of finasteride for at least 3 months.
The following factors were the exclusion criteria: bearers of diseases with systemic hormonal alterations (for example hypothyroidism, hematological pathologies, diabetes mellitus, cancer, hypertension, patients in use of hormone-acting drugs, and patients with platelet levels below 130,000.
The participants of the study had the sides of the scalp randomized to receive either PRP or placebo. A computerized system was used to perform the randomization and to ensure the secretiveness of the sides draw. Both patients and the evaluator physician were blinded.
Three consecutive monthly sessions were performed, with subcutaneous injections of PRP and placebo, each applied on one of the sides of the scalp.
The PRP was obtained from autologous blood, meaning that each patient supplied his own blood for the preparation of the infusion to be applied into his own scalp. A 45 ml sample of whole blood was collected in the presence of anticoagulant, whose composition does not damage the platelets (sodium heparin). This sample was subjected to a double and continuous centrifugation process, during which a volume of 45 ml of whole blood was inoculated into a single 50 ml capacity tube, in a fully enclosed environment and isolated from the external air. The tubes were centrifuged at room temperature, resulting in three basic components: red cells, platelet-rich plasma (PRP), and platelet-poor plasma (PPP). The PRP volume of roughly 5ml was collected within the double tube, specifically developed for that end, with 4ml of 10% calcium chloride being subsequently added. The material was then infused subcutaneously on the previously randomized side of the scalp.
The evaluation of the primary outcome was performed using the Trichoscale® software (FotoFinder Systems, Inc., Columbia, Maryland, USA). The software is runs by the FotoFinder® device, which is a digital dermoscopy system developed by a German company in conjunction with the Tubigen University in Germany, and which magnifies cutaneous lesions by 20 to 70 times. The software component was developed for a more accurate analysis of the scalp, and builds a digital trichogram. It is able to evaluate the following parameters: hair density (strands per square centimeter), percentage of anagen and telogen strands, vellus and terminal hair densities, and measurement of follicular units. The evaluation performed by the software was carried out on previously established and standardized areas: two circular areas with 1.5cm in diameter, located in the parietal region of each side of the skull, 14cm from the mastoid process on the respective side. The evaluation was carried out on three timepoints: 15 days before the first application, and at 30 and 60 days after the end of the treatment.
Secondary outcomes were determined by clinical and photographic evaluations of the scalp. In addition, the authors of the present article assessed the procedure's safety by recording the adverse events that were reported on all scheduled encounters (treatment and follow-up visits).
Of the 8 patients selected, one dropped out and another did not attend the last PRP application session.
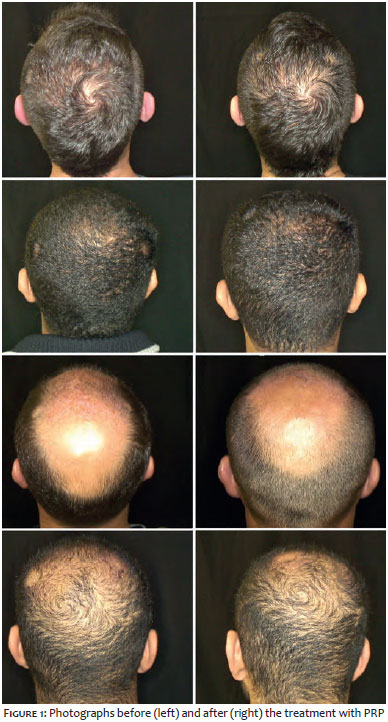
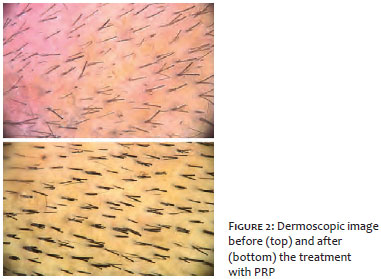
The 6 patients who received the complete treatment noticed some degree of improvement, especially regarding the hair loss. The photographic assessment can be seen in Figures 1 and 2.
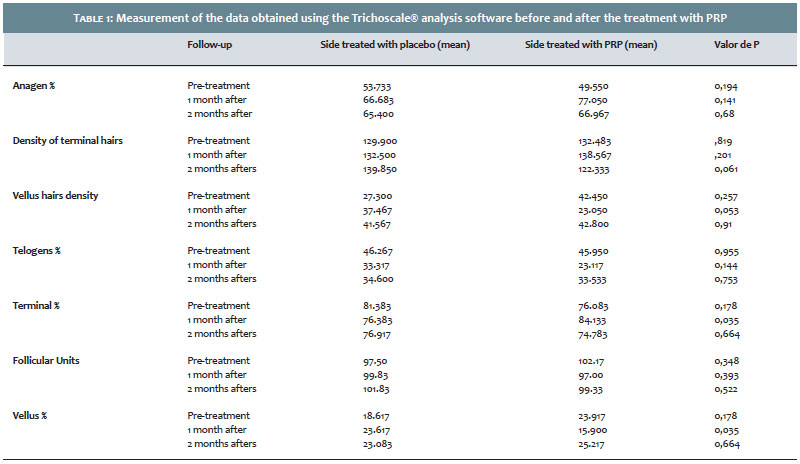
The results from the statistical analysis of the data performed by the Trichoscale® software are presented in Table 1, with a comparison of the mean values obtained from the sides treated with PRP and placebo. The Student t-test was used in order to obtain the results mean values.
Based on the analysis of Table 1, it is possible to infer that there was an increase in the percentage of anagen strands and a reduction in telogen strands in both of the treated sides, however the improvement was more significant on the PRP side. Both the increase in anagen hairs and the decrease in telogen hairs continued in the second month after treatment.
Furthermore, there was a statistically significant reduction in vellus hairs (p = 0.035) on the PRP side after the first month of treatment, however this reduction was not maintained in the second month.
Regarding the terminal hairs, there was an important increase in the PRP side, with statistical significance (p = 0.035) after the first month of treatment. The result was not maintained in the second month.
Regarding adverse effects, the only symptom reported by the patients was pain during the application, being that 4 patients reported pain a few hours after the application. Even though, the pain was rated as tolerable by the patients, and there was no need for analgesia even for those who complained of pain after the procedure. No signs of erythema, edema or heat sensation was observed in the application site.
Platelet-rich plasma contains growth factors that have effects on the cells' maturation and the wound repair process. Its use in wound repair, and orthopedic and cardiac surgeries is growing increasingly. In the treatment of androgenetic alopecia, PRP has been studied with good prospects to emerge as an effective and safe treatment.
A study by Gentile et al with a sample of 23 patients compared the injection of PRP on one side versus placebo on the other side, for treatment of androgenetic alopecia. After 3 monthly cycles of treatment, the patients showed clinical improvement in the average number of hairs per analyzed area. A microscopic evaluation evidenced increased epidermal thickness and number of hair follicles. There was also an increase in Ki67 (a marker of cell proliferation), in epidermis' keratinocytes, and in follicle bulge cells. 4
Another study, carried out by Singhal el al., tested the infusion of PRP in the scalp of 8 patients diagnosed with androgenetic alopecia, while the control group received a different drug therapy. In the PRP group, there was hair growth after 12 weeks of treatment and a reduction of 65% in the hair traction test. The control group did not experienced the same outcomes.5
A prospective cohort study of 20 patients with the application of PRP every 21 days and a new small volume application after six months showed a reduction in hair loss, which after 3 months reached normal levels. Furthermore, it was possible to notice increased hair density as compared to the baseline. 6
A study conducted by Schiavone et al. with 64 male and female patients with androgenetic alopecia analyzed the application of two injections of leukocyte plasma rich in platelets (L-PRP) with the addition of concentrated plasma proteins. Two independent evaluators assessed photographs taken at baseline and after 6 months. Some degree of improvement was observed in all patients by one of the evaluators while the other identified improvement in 62 patients. In this study, it was possible to observe that the proposed treatment can induce some degree of clinical improvement for the male and female baldness.7
The great potential of PRP is linked to the concentration of growth factors contained in platelets. Many of them are involved in the regulation of morphogenesis and hair growth, and in the cyclic transformation of the hair follicle, acting as biological switches that are turned on and off during the different phases. 5.8 The main growth factors involved in the hair follicle growth are: vascular endothelium growth factor (VEGF), epidermal growth factor (EGF), insulin-like growth factor (IGF), and fibroblast growth factor (FGF). Platelets release large amounts of growth factors derived from platelets (PDGF), EGF and VEGF.5
Activated PRP seems to promote the differentiation of hair follicular stem cells through the stimulation of b-catenin transcription activity. In addition, it induces the in vitro proliferation of dermal papilla cells, increasing the growth of cells through the activation of kinase-dependent extracellular signaling (ERK). Platelet-rich plasma also appears to prolong the anagen phase of the hair growth cycle by increasing the expression of the fibroblast growth factor 7 (FGF-7), and to increase cell survival via the inhibition of apoptosis. 1 Another mechanism of action is the increase in the levels of VEGF and PDGF, stimulating angiogenesis in the perifollicular vascular plexus. 3.5
The results of the present study were obtained through the dermoscopic analysis evaluated by the Trichoscale® software. There was an increase in anagen hairs, with a reduction of telogen and vellus hairs, and an increase in terminal hair. The results were statistically relevant for the reduction in vellus hairs and the increase in terminal hairs. The evaluation also included a 2-month follow-up after the treatment. Failure to maintain good results in this follow-up may be related to the androgenic hormonal stimuli that act on the progression of the disease. That fact contributes with the hypothesis that PRP therapy could be indicated as an adjuvant treatment in androgenetic alopecia. Also, there was an improvement on the side treated with placebo, which could be explained by the PRP's action from distance.
The present study's advantage was that the used PRP material was prepared according to a protocol, as described in the "Methods" section. For the evaluation of results, the authors used dermoscopic images analyzed by the Trichoscale® software, an assessment method that is more objective than the isolated photographic analysis.
The limitations of the present study were the small number of participating patients and the fact that the outcomes were not followed-up more prolongedly.
Androgenetic alopecia is a frequent complaint in the dermatology practices. There are several established treatments; however obtaining an effective treatment is still a challenge.
In the present study, a clinical improvement evidenced by photographs was observed, and positive results were documented by the Ttrichoscale® analysis. There was statistical relevance in the data obtained, especially after the first month of treatment.
In light of the results obtained and the considerable therapeutic potential of platelet-rich plasma, the authors of the present study believe that this new therapeutic resource will certainly add up to the dermatologists' armamentarium for the treatment of androgenetic alopecia.
Further studies should be carried out aiming at scientifically evidencing PRP's real effectiveness.
1. Li ZJ, Choi HI, Choi DK, Sohn KC, Im M, Seo YJ, et al. Autologous platelet-rich plasma: A potential therapeutic tool for promoting hair growth. Dermatol Surg. 2012;38:1040-6.
2. Maria-Angeliki G, Alexandros-Efstratios K, Dimitris R, Konstantinos K. Platelet-rich plasma as a potential treatment for noncicatricial alopecias. Int J Trichol 2015;7:54-63
3. Arshdeep, Kumaran MS. Platelet-rich plasma in dermatology: Boon or a bane? Indian J Dermatol Venereol Leprol. 2014;80:5-14.
4. Gentile P, Garcovich S, Bielli A, Scioli MG, Orlandi A, Cervelli V. The Effect of Platelet-Rich Plasma in Hair Regrowth: A Randomized Placebo-Controlled Trial. Stem Cells Transl Med. 2015;4(11): 1317-23
5. Singhal P, Agarwal S, Dhot PS, Sayal SK. Efficacy of platelet-rich plasma in treatment of androgenic alopecia. Asian Journal of Transfusion Science. 2015; 9 (2):159-62.
6. Gkini MA, Kouskoukis AE, Tripsianis G, Rigopoulos D, Kouskoukis K. Study of platelet-rich plasma injections in the treatment of androgenetic alopecia through a one-year period. J Cutan Aesthet Surg. 2014;7:215-21
7. Schiavone G, Raskovic D, Greco J, Abeni D. Platelet-Rich Plasma for Androgenetic Alopecia: A Pilot Study. Dermatol Surg. 2014 (40): 1010-19
8. Lin WH, Xiang LJ, Shi HX, Zhang J, Jiang LP, Cai PT et al. Fibroblast Growth Factors Stimulate Hair Growth throughbβ -Catenin and Shh Expression in C57BL/6 Mice. Biomed Res Int. 2015;2015: 9p.
This study was performed at Universidade de Mogi das Cruzes (UMC) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}