


Daniel Dal'Asta Coimbra1; Betina Stefanello de Oliveira2
Introduction: The evolution of filling techniques allowed a three-dimensional approach to the face: nowadays volumetric restoration is more important than grooves.
Objective: Description of an unpublished technique of facial volumization through the injection of filler in the supra-auricular region, with a detailed review of the regional anatomy.
Methods: A retrospective case-control study was conducted in patients presenting skin mobility in the temporo-parietal region. The injection of Hyaluronic Acid for volumetric replacement was done using cannulae, bolus and fan techniques in the supra-auricular region, limited antero-superiorly by the area of ¿¿hair implantation and inferiorly by the tragus. The patients were evaluated clinically, photographed and had their data analyzed by statistics.
Results: 152 women and 13 men aged 24 to 84 years were treated between July and September 2016. The volume of Hyaluronic Acid used in the patients ranged from 0.6 to 2.6 ml. In 8 cases local edema was observed due to hematoma during application, that was controlled by digital compression. Significant improvement of the facial contour was observed.
Conclusion: The use of fillers in the supra-auricular region allows a three-dimensional approach and promotes static and dynamic rejuvenation of the entire face.
Keywords: DERMAL FILLERS, HYALURONIC ACID; REJUVENATION
Beauty is a characteristic – or set of characteristics – that are pleasant to the eye and capable of captivating the observer. The concept of beauty varies according to the culture and personal opinion. Nevertheless, proportionate, symmetrical, well-marked faces with rounded contours and high cheeks appear to be more attractive. 1
The rhytidectomy has always been considered the gold standard in the treatment of facial sagging and in the promotion of facial rejuvenation since its emergence at the beginning of the 20th century. 2 In 1920, Bettman improved the technique, describing the pre-auricular and temporal access that led to a more unnoticeable scar, similar to those obtained nowadays. Over time, the development of techniques has brought increasingly natural results, however, as a consequence of the risks, and the definitive and not always satisfactory outcomes, the surgical approach is limited to treating the consequences of aging in the vast majority of cases. 3,4
During the last decades, there has been a better understanding of the facial aging process, specially regarding the knowledge about fat compartments 5.6 and the measurement of facial bone remodeling. 7 Concomitantly, new filling substances have been developed aimed at restoring the volume, while botulinum toxin began to be employed for the reeducation of muscles. As a result, a new era was established in the facial rejuvenation treatment, where non surgical liftings have been standing out, yielding outcomes that are both surprising and natural.1,8,4,9
The search for filling substances that are safe, long lasting, and whose effects are predictable and natural, has led to hyaluronic acid (HA), which is a polysaccharide (glycosaminoglycan compounded by alternating and repetitive units of D-glucuronic acid and N-acetyl-D-glucosamine) with hydrophilic properties, which causes an increase in the injected tissue. 10.11 The initial filling effect is directly related to the volume of filler injected; however, studies have demonstrated that there is an indirect effect when it is injected into the dermis due to the activation of fibroblasts. The need for a filler aimed at deep applications in the face (fat compartments and/or juxta-periosteum) led to the development of volume restoration-specific HA, 12 which have higher concentrations of HA and crosslinking than the HA fillers used in the dermis or superficial subcutaneous. This brought increased durability and viscosity to the gel, generating an increase in its lifting capacity against the skin's pressure. 11 The duration of the HA based fillers and of those aimed at restoring volume in general ranges from 12 to 24 months. 10
The search for natural results has led to the development of different facial rejuvenation treatment techniques using fillers (e.g. MD Codes®) in order to avoid distortions, exaggerations or overcorrections that are very often observed when the wrong techniques are employed. 4,13 Nowadays, in addition to the three-dimensional static improvement of the face, the maintenance or improvement of facial motion stand out in facial rejuvenation treatments with fillers, with facial expressions being key in the choice of the application sites. In this way, applications cease to be static and become dynamic three-dimensional procedures based on the facial mimicry, where the filling material can hinder muscle contraction by mechanical block or facilitate the muscle movement via a deep support effect, reducing the force needed for the muscle to exert contraction. 13.14
The ear is disposed over the temporal bone. The temporal region is formed by the temporal bone, which articulates with the occipital, parietal, zygomatic, sphenoid and mandible bones.
The temporal region's tissue layers are: skin, subcutaneous fat, superficial temporal fascia (STF), deep temporal fascia (DTF) and temporal muscle. The STF is the continuation of the superficial muscular aponeurotic system (SMAS) of the face and the galea aponeurotic system of the scalp. This multilaminated fascial layer (also called temporoparietal fascia) is loosely adhered to the subcutaneous fat and is closely associated with the frontal branch of the facial nerve and the superficial temporal vessels. The loose areolar tissue, denominated subaponeurotic plane, separates the STF from the DTF and is the dissection plane that is commonly used in surgical approaches of the temporal region.
The DTF is a dense conjunctive tissue layer adhered to the superior temporal line that covers the temporal muscle. A few centimeters above the zygomatic arch, the DTF splits into superficial and deep layers. Between these two layers is the superficial temporal fat pad, which is irrigated by the middle temporal artery. In the direction of the DTF's deep layer lies the deep temporal fat pad, corresponding to the superior extension of the buccal adipose body. This extension runs superiorly and deeply regarding the zygomatic arch, to lay between the DTF's deep layer and the temporal muscle. 15, 16
The superficial temporal artery and the temporal branch of the facial nerve are two noble anatomical structures that should be well known for the approach of this region with the use of fillers.
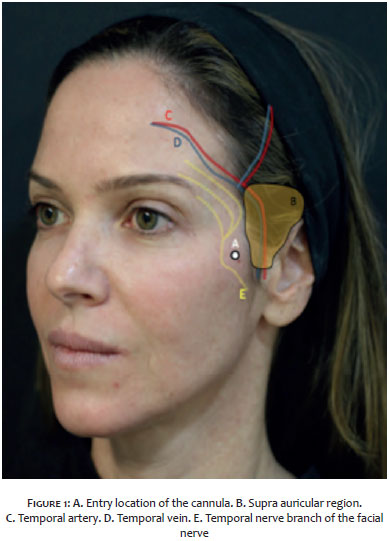
The superficial temporal artery is the terminal branch of the external carotid artery. It originates within the parotid gland, rising roughly 10mm anteriorly to the tragus, to cross the zygomatic arch. The superficial temporal artery gives rise to numerous terminal branches, including the facial transverse, the medial temporal, the parietal and the frontal branches (Figure 1). 16,17
The temporal branch of the facial nerve emerges from the superior margin of the parotid gland 1.7 cm anteriorly to the tragus, and crosses the zygomatic arch to supply the superior auricular and the anterior auricular muscles, the frontal part of the occipitofrontalis muscle, and, most importantly, the upper orbicularis muscle of the eye. The temporal nerve, which runs close to the deep face of the STF, is located superficially when it crosses the zygomatic arch and is loosely adhered to the adjacent facial layers. The vulnerability of the temporal branch is located at the level of the middle third of the zygomatic arch. Its path continues towards the frontotemporal region, always close to the deep face of the SMAS, up until penetrating the frontal muscle in its deep face. Its lesion causes palpebral ptosis and permanent difficulty to raise the eyebrow.18 (Figure 1)
To describe an unprecedented technique of non-surgical facelift based on the application of volumetric replacement HA cutaneous filler in the supra auricular region, promoting beneficial changes in the motion of the facial mimicry and rejuvenating the entire face.
A retrospective case-control study was performed for the introduction of an unpublished technique of supra-auricular cutaneous filling aimed at performing a pan-facial facelift, carried out at the private practice of one of the authors, in the city of Rio de Janeiro (RJ), Brazil, from July to September 2016.
A total of 165 patients who sought care with indication for treatment of improvement of the facial contour received cutaneous filler in the supra-auricular region, having been distributed according to the Venn diagram in Figure 2.
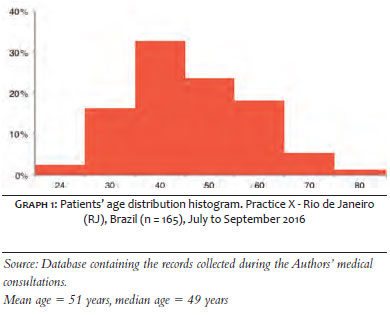
Of these, 152 patients were women, and 13 were men. Their ages ranged from 24 to 84 years (mean = 51 years, median = 49 years) (Graph 1).
For the selection of the patients, a test was carried out by stretching the skin from the temple towards the parietal region using the index finger's pulp. The patients who experienced motion in this tissue were included in the study for the filling of this region. There was no restriction regarding gender, age or phototype. Thirty-three patients (20%) had already undergone rhytidectomy. The study complied with the ethical directives of the 2000 Helsinki Declaration.
With the patient lying down at 60 degrees, asepsis was carried out with 2% alcoholic chlorhexidine solution on the entire face and the temporal region covered by the hair. Next, an orifice was performed so as to allow the cannula to enter the temporal region, over the zygomatic bone. A 24G or 25G cannula was inserted through the orifice and slid through the subcutaneous up until it reached the supra-auricular region, where a bolus of 0.1 to 0.2ml of volumetric replacement HA was injected with lidocaine into the subcutaneous tissue. Digital pressure was then exerted on this bolus in order that the dispersion of the product produced anesthetic effect in the region. This was followed by the application of a new volume of the substance, using the fan technique, applying little force and with slow, gentle movements in the entire supra auricular area – with the area of hair implantation being the antero-superior limit, and the tragus, the inferior limit (Figure 1). A greater amount of the product was deposited in the region closer to the ear, in a more depressed area easily demarcated by digital palpation.
Due to the lifting effect produced by this lateral application, there was flattening and decreased anterior projection of the zygomatic region in some patients. In these patients, after the supra-auricular application, 0.33 ml of the product, on average, were injected on each side at the point of greatest anterior projection of the Zygomatic bone, using the same orifice for the introduction of the cannula, but this time moving it towards the anterior region of the face.
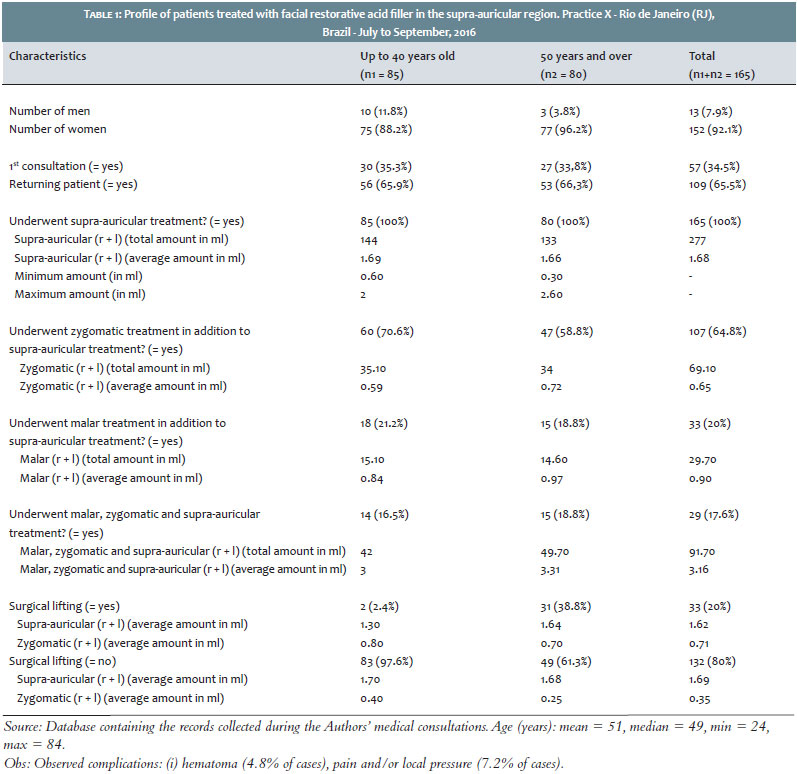
A total of 165 patients were treated (152 women = 92%, 13 men = 8%). Their ages ranged from 24 to 84 years (mean = 51 years). Of these patients, 33 (20%) had already undergone facelift (Table 1). A total of 57 (34.5%) patients were seeking care for the first time, while 108 (65.5%) had previously attended consultations.
The total amount of product injected in the supra auricular region ranged from 0.6 ml to 2.6 ml, with an average of 1.68 ml (total injected volume). There was no statistical correlation between age and amount of product applied. In 107 patients (64.9%), it was necessary to complement the product in the zygomatic region with a mean volume of 0.33 ml per side.
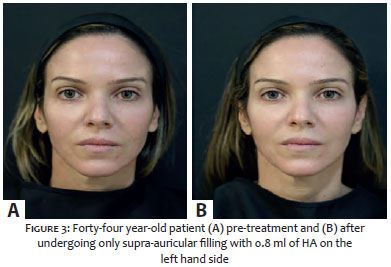
After the application, a significant improvement of the entire facial contour was observed, related to the lifting effect caused by the product deposited in the treated region. In addition, there was improvement and softening of the facial expressions, generating static and dynamic rejuvenation in the entire face, which was very evident when a treated hemiface is compared with the contralateral hemiface before the treatment (Figure 3).
Despite the fact that block or topical anesthetic were not used, patients reported only mild pain, with a few patients who had previously undergone surgical facelift at the site regarding it as moderate. Edema in the region was reported as imperceptible and in 8 cases there was presence of local bulging due to hematoma during the application, which were immediately controlled by digital compression, not having externalized in the skin on the days following the procedure. All patients realized improvement in the photographic evaluation performed immediately after the procedure, having been instructed to return to their normal activities. No paradoxical depression of the temple was observed due to a possible excess of product in the supra-auricular region.
The search for naturalness in facial rejuvenation, associated with a better understanding of the aging process and the development of new techniques and volumetric replacement HA based fillers, have led to increasingly extraordinary results, often compared to those obtained only through surgical facelifts.
The three-dimensional approach of the face with the use of fillers is a safe method that yields natural and long lasting outcomes when adequately used. A thorough knowledge of each region's anatomy and changes linked to the aging process is of paramount importance so that the treatment can early address the causes – such as volume replacement in the fat pads or in juxta-osseous locations – in order to avoid, attenuate or postpone consequences arising on the surface, such as lines and furrows in the skin. Currently, in addition to this static three-dimensional improvement of the face, the maintenance or improvement of the facial motion has stood out in rejuvenation treatments with fillers, where facial expressions are key in the choice of the application sites.
After six years using volumetric replacement AH fillers with a three-dimensional approach of the entire face, a total of 7,194 ml of Juvederm Voluma® (Allergan Inc., Irvine, USA) have been applied in the upper, middle and lower thirds of patients' faces, in procedures carried out at one of the present study's authors' private practice, located in the city of Rio de Janeiro (RJ), Brazil. Initially the applications were mainly focused on the improvement of the shadow areas, concavities and projection of the lower contour of the face, in a static way. The practice with the use of fillers, the improvement of the technique, as well as the personal experience of the injector physician in the treatment of patients with facial paralysis using fillers resulted in the development of a dynamic three-dimensional approach. More recently, this approach led to the description of the treatment of the body site described in the present study, which is unprecedented in the world literature, thus being now considered by the authors as the first and most important facial region for volumetric replacement.
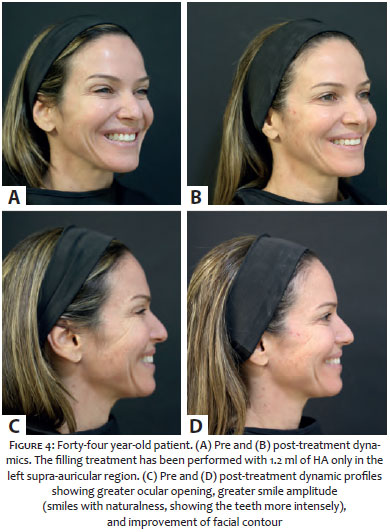
Based on the palpation of a depressed area in the temporal region covered by hairs and the lifting effect caused by the digital traction of the skin from that area towards the parietal region, it was possible to verify that the patients could benefit from the volumetric replacement with HA at that body site. Using the technique described above, the authors of the present article performed the application of the product in the site, with an immediate lifting effect occurring in the entire face, in addition to a decrease in the ptosis of the malar and nasolabial fats above the nasolabial folds, an increase of the cutaneous tension in the lower eyelid due to lateral traction, the elevation of labial commissures, and the improvement of the mandibular contour. In addition to these static effects and for the surprise of the authors, there was an elevation in the brow's tail, given that during the smile, a greater amplitude of the mouth was generated (greater exposure of the lateral teeth) and an increase in the ocular opening, probably due to the decrease in the need for using the upper lip elevator muscle, in addition to a slight decrease in the hypertrophic platysmal bundles, promoting a non-surgical Dynamic Three-dimensional Lifting®. (Figures 4 and 5)
As already mentioned, the authors did not find any report of similar technique in the literature, with the three-dimensional approaches linked to filler injection based rejuvenation that have already been described usually beginning in the zygomatic and malar regions. 4,12 The approach proposed in the present study is unpublished and differs from those that have been studied in that the middle third's volumization begins in the supra auricular area covered by the hair, which is an almost imperceptible, safe area when the correct technique is employed – and practically painless when HA is used with lidocaine in its formulation. The possibility of immediately returning to daily activities provided a high degree of patient satisfaction. In addition, the facelift effect generated by the filler in this new area led to a decrease in the amount of AH needed in the zygomatic and malar regions, which generated less anterior projection of the face and extremely natural outcomes both statically and during facial mimicry.
Due to the lateral traction caused by the supra-auricular filling, 64% of patients presented a slight flattening and decrease of the anterior projection of the zygomatic region. In these patients, after the supra-auricular application, small volumes (on average 0.33 ml) of AH were injected into the zygomatic region on each side on the same occasion. It is important to note that the aging process is dynamic and occurs throughout the face, and other regions can be treated with fillers on the same occasion or in new sessions, depending on the needs of each face. After treatment of these regions, some patients were also treated in the malar region and in the upper and lower thirds of the face, however in the present study the authors considered only the influence of volume replacement in the supra auricular region in the middle facial third. (Table 1) Despite the fact that the authors use a considerable amount of the product (on average 0.84 ml on each side), they have not observed paradoxical depression of the temples, given that the treated area is covered by hair.
Of the patients treated, 57 (34.5%) had sought care for the first time, while 108 (65.5%) were patients who had already been previously seen. Comparing the two groups, the amount of product injected into the supra auricular region was lower in the new patients (1.57 as compared to 1.74 ml), nonetheless the concomitant treatment of the zygomatic and malar regions was significantly more frequent in the new patients group (84.2% as compared to 54.6% in patients also treated in the zygomatic region, and 40.4% as compared to 5.6% in those who were treated both in the zygomatic and malar regions). It was probably in the group of patients who had previously been seen and undergone treatment with fillers that there was less need to treat the zygomatic and malar regions, since they had already been treated in these regions before this new area has been described. These data demonstrate the importance of evaluating and treating the entire middle third of the face, especially in patients who have not undergone facial volumization, with the ideal treatment sequence proposed by the authors of the present article is to start with the supra auricular region, move on to the zygomatic, and finally treat the malar area.
Due to the important vascular-nervous structures present in the temporal region, the authors of the present study believe it is essential to use cannulas for the application of the product.19 The choice to enter via an orifice over the zygomatic bone entails that the cannula will have to travel a path perpendicular to the large vessels (temporal artery and vein), which would minimize the risk of intravascular injection. The movements should be slow and gentle, and aspirations can be made if there is any doubt as to the positioning of the cannula in relation to the vessels.20 The authors of the present study chose 24 and 25G cannulas based on their personal injecting experience, however cannulas of greater caliber can be used. Cannulas 27 and 30G should be avoided due to the increased risk of vascular accidents.21,22
The predominance of the female gender in the sample can be explained by the fact that the search for aesthetic procedures is still more frequent among women. The age ranged from 24 to 84 years, indicating the versatility of the filling procedure, which can be performed as long as the clinical examination identifies the need for it. In the experience of the author of the present study, young faces and still with little mobility of the skin at the site required smaller amounts of the product, however in the study's sample there was no statistical correlation between the age and the amount of product applied. The complex TMJ (temporomandibular joint) is located in the temporal region, and due to its almost constant motion and contraction, it is an area that undergoes intense bone remodeling and fat resorption, which justifies the treatment of this region even in young patients.
Of the study patients, 20% had already undergone a surgical facelift. In general and despite the cutaneous mobility present at the clinical examination, there was greater resistance to the passage of the cannula in the subcutaneous of these patients. In the studied sample, patients who had previously undergone surgical facelifts required treatment in the zygomatic region with significantly greater amounts when compared to those who had not undergone surgery (0.71ml x 0.35ml). Seven (87.5%) of the 8 patients who presented hematoma during the procedure – probably due to lesion to the temporal vein – had undergone surgical facelift at the site.
The choice for volumetric replacement AH (Juvederm Voluma® Allergan Inc., Irvine, USA) was based on the fat that the treated region is an area with great osteoarticular mobility, demanding a malleable product, however with a great capacity for lifting and deep tissue support. Further studies with hyaluronic acids from diverse brands should be carried out aimed at reproducing the results obtained in the present study.
Finally, due to the fact that the technique introduced by the present article is a recent and unprecedented, it is not yet possible to estimate the duration of the product's permanence in this region. Thus, further studies are needed to evaluate the long run results of supra auricular filling.
The authors of the present study have described a new technique for the three-dimensional rejuvenation of the face using fillers, in which volumetric replacement AH applied in the supra-auricular region promotes a non-surgical pan-facial lifting effect, with static and dynamic facial improvement. This new region is part of what the authors of the present study have termed Dynamic Three-dimensional Lifting® with the use of fillers, where the volumizing approach is based on facial mimicry. This description may serve as a platform for further studies related to the better understanding of the effect of fillers in the process of static and dynamic aging.
The Authors of the present article would like to particularly thank the biostatistician and physician Dr. Luiz Felipe Pinto for contributing in the review of data and statistical analysis, and Natalia Caballero Uribe for the illustrations.
1. Coimbra DD, Uribe NC, Oliveira BS. "Quadralização facial" no processo do envelhecimento. Surg Cosmet Dermatol. 2014;6(1):65-71.
2. Neligan PC. Plastic surgery: 6 volume. 3rd ed. St. Louis, MO: Elsevier Saunders; 2012.
3. Kim YB. The History and Future of Plastic and Reconstructive Surgery. Arch Plast Surg. 2015;42(5):515-6.
4. Maio M. The minimal approach: an innovation in facial cosmetic procedures. Aesthetic Plast Surg. 2004;28(5):295-300.
5. Gierloff M, Stöhring C, Buder T, Gassling V, Açil Y, Wiltfang J. Aging changes of the midfacial fat compartments: a computed tomographic study. Plast Reconstr Surg. 2012 129(1): 263-273.
6. Pessa JE, Rohrich RJ. Discussion: Aging changes of the midfacial fat compartments: a computed tomographic study. Plast Reconstr Surg. 2011;129(1):274-5.
7. Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation age-rela- ted changes of the orbit and midcheek and the implications for facial rejuvenation. Aesthet Plast Surg. 2012;36(4):753–60.
8. Coimbra DD, Oliveira BS, Uribe NC. Preenchimento nasal com novo ácido hialurônico: série de 280 casos. Surg Cosmet Dermatol 2015;7(4):320-6.
9. Carruthers J, Carruthers A. Técnicas de Preenchimento. New York: Elsevier; 2005.
10. Carruthers J, Cohen SR, Joseph JH, Narins RS, Rubin M. The science and art of dermal fillers for soft-tissue augmentation. J Drugs Dermatol. 2009;8(4):335-50.
11. Carruthers J, Carruthers A, Tezel A, Kraemer J, Craik L. Volumizing with a 20 mg/ml smooth, highly cohesive, viscous hyaluronic acid filler and its role in facial rejuvenation therapy. Dermatol Surg, 2010;36 Suppl 3: 1886-1892.
12. Raspaldo H. Volumizing effect of a new hyaluronic acid sub-dermal facial filler: a retrospective analysis based on 102 cases. J Cosmet Laser Ther. 2008;10(3):134-42.
13. Cotofana S, Schenck TL, Trevidic P, Sykes J, Massry GG, Liew S, Graivier M, Dayan S, de Maio M, Fitzgerald R, Andrews JT, Remington BK. Midface: Clinical Anatomy and Regional Approaches with Injectable Fillers. Plast Reconstr Surg. 2015;136(5 Suppl):219S-234S.
14. Sapijaszko MJ. Dermal fillers: Ever expanding options for esthetic use. Skin Therapy;12(8):4-7.
15. Breithaupt AD, Jones DH, Braz A, Narins R, Weinkle S. Anatomical Basis for Safe and Effective Volumization of the Temple. Dermatol Surg. 2015;41 Suppl 1:S278-83.
16. Salasche S, Bernstein G, Senkarik M. Surgical anatomy of the skin. New York: Appleton & Lange; 1988. 200-15.
17. Tamura BM. Anatomia da face aplicada aos preenchedores e à toxina botulínica – Parte II. Surg Cosmet Dermatol. 2010;2(3):205-14.
18. Silva MLA; Aboudib JH; Castro CC. Anatomia aplicada do ramo temporal do nervo facial: estudo do risco potencial de lesão durante a cirurgia do rejuvenescimento facial. Rev. Bras. Cir. Plást. 2010;25(4):604-613.
19. Vartanian AJ, Frankel AS, Rubin MG. Injected hyaluronidase reduces restylane-mediated cutaneous augmentation. Arch Facial Plast Surg. 2005;7(4):231-7.
20. VIiana GAP, Osaki MH, Cariello AJ, Damasceno RW. Tratamento dos sulcos palpebromalar e nasojugal com ácido hialurônico. Arq Bras Oftalmol. 2011;74(1):44-7.
21. Bellman B. Complication following suspected intra-arterial injection of Restylane. Aesthet Surg J. 2006;26(3):304-5.
22. 22. Lowe NJ. Arterial embolization caused by injection of hyaluronic acid (Restylane). Br J Dermatol. 2003;148(2):379; author reply 379-80.
This study was performed at Dr. Daniel Dal'Asta Coimbra's private practice, Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}