


Guilherme Bueno de Oliveira1; Natália Cristina Pires Rossi2; Gustavo Bueno de Oliveira3
Introduction: Hyperhidrosis is a common disease characterized by excessive sweating. Several treatment options are described as axillary liposuction and laserlipolysis.
Objective: To compare the effectiveness of two treatment methods for axillary hyperhidrosis – one exclusively surgical (liposuction) and the other employing invasive laser therapy (laserlipolysis) – using a prospective, comparative study with a one-year follow up.
Methods: Liposuction was carried out in the right axilla, while laser lipolysis was performed in the left axilla. The evaluation was conducted using the starch-iodine test, comparative histological analysis and patient self-assessment questionnaires.
Results: Twelve patients took part in the study. The starch-iodine test indicated decreased sweating in all patients within one year after the procedures, while the histological analyses showed absence or reduction of the secreting ducts and acini on both sides and in all cases. After one year of follow-up, the patient's satisfaction index measured by the questionnaires remained positive in all cases, with 75% asserting maximum satisfaction, and 25% reporting difference between the sides (better results were described in the right hand side axilla).
Conclusions: Both techniques showed similar effectiveness after one year of follow-up. Laserlipolysis had a lower frequency of postoperative complications.
Keywords: LASERS; LASER THERAPY; DERMATOLOGY; DERMATOLOGIC SURGICAL PROCEDURES
Hyperhidrosis is a common condition characterized by excessive sweating. It can manifest in one or more areas: axillae, palms, face, scalp, soles, and groin. 1 Excessive production of sweat – more than necessary to regulate the body's temperature – can significantly influence the affected patients' quality of life, possibly leading to depression or social isolation. Hyperhidrosis can be classified as primary, secondary, generalized (whole body) or focal (specific body sites). 1,2
Primary axillary hyperhidrosis (PAH) is idiopathic and focal. In addition to affecting the patients' quality of life, it can also lead to a variety of complications, such as bacterial or fungi overgrowth, muscle cramps, eczematous dermatitis, and other dermatological conditions. 3 Secondary hyperhidrosis can be generalized or focal, and results from some triggering event, such as endocrinopathies, neuropathies, infections etc. 1-3 Several treatment options are available for the treatment of axillary hyperhidrosis: topical antiperspirants, systemic medications, iontophoresis, botulinum toxin type A, eccrine glands curettage, axillary liposuction, laserlipolysis, radiofrequency, 3,4 and microwave. 5.Cases should be evaluated on an individual basis in light of the severity, the picture's extension, and advantages and disadvantages of each method. Conservative treatments should be given priority. 1
The liposuction of eccrine glands is a procedure aimed at aspirating the axillary region's glands, and is performed under local tumescent anesthesia. Laserlipolysis is based on the emission of 915nm wavelength diode laser beams, which stimulate heat in the axillary region, leading to the destruction of sweat glands, in turn interrupting its production at once and definitively. 1-4
The present paper describes a prospective, comparative and monocentric study aimed at comparing the effectiveness of two approaches for treating axillary hyperhidrosis: an exclusively surgical method (liposuction) and another based on invasive laser therapy (laserlipolysis).
Patient selection
Twelve patients bearing primary axillary hyperhidrosis who underwent prior treatment with topical antiperspirant and botulinum toxin type A injections were selected. Only patients who had similar intensity of hyperhidrosis in both axillae (verified by the starch-iodine test) were included. The study complied with the Declaration of Helsinki's ethical principles.
The group's epidemiological analysis was conducted based on the following factors: age, gender, and complications during and after surgery.
Exclusion criteria
Patients with conditions that could stimulate hyperhidrosis, those who used drugs that stimulated sweating, or who had undergone thoracic sympathectomy or another surgical method to treat hyperhidrosis were excluded.
1. Hyperhidrosis quantification test
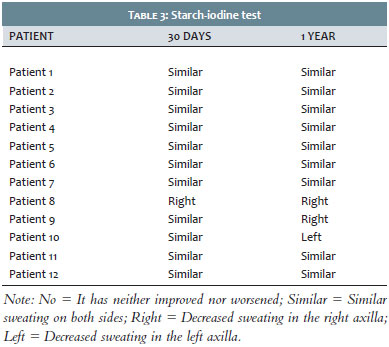
The starch-iodine test comprises the application of iodine solution in the sweating area, followed by drying and subsequent spraying of starch on the same zone. The combination of starch and iodine with sweat lends a dark blue color to the region. This test was performed before, 30 days after, and one year after the procedure. The difference between the sides received the following classification:
No = It has neither improved nor worsened
In case of improvement:
Similar = Similar sweating on both sides
Right = Less sweating on the right
Left = Less sweating on the left
2. Histological analysis
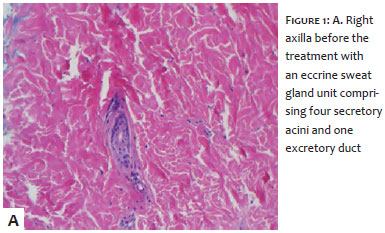
Histology was performed on both axillae after biopsy with 5mm punch in the axillary cavities (intersection of the horizontal and vertical middle axillary lines) before the procedure and 30 days later. The objective was to identify the area with the greatest number of glands (acini and ducts) in a fixed observation field.
3. Satisfaction questionnaires
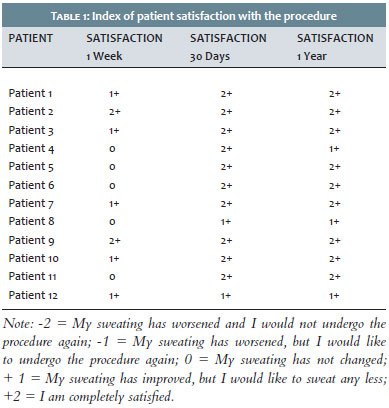
The patients answered a questionnaire about their degree of satisfaction with the procedures 1 week, 30 days and 1 year after the procedures were performed, using the ratings below:
-2 = My sweating has worsened and I would not undergo the procedure again
-1 = My sweating has worsened, but I would like to undergo the procedure again
0 = My sweating has not changed
+1 = My sweating has improved, but I would like to sweat any less
+2 = I am completely satisfied
4. Questions about the difference in the results obtained for each side
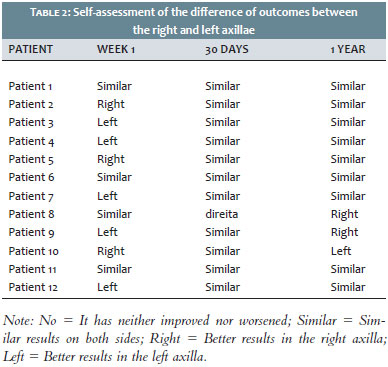
The patients answered a second questionnaire 1 week, 30 days and 1 year after the procedure, aimed at subjectively quantifying the difference between the sides, using the following ratings:
No = It has neither improved nor worsened
In case of improvement:
Similar = Similar results on both sides
Right = Better results in the right axilla
Left = Better results in the left axilla
Statistical analysis for the assessment of the difference in outcomes using diverse techniques
The statistical analysis of this correlated paired sample was performed based on the results obtained with starch-iodine test, using Microsoft Excel's McNemar test with continuity correction, and a 5% significance level (alpha = 0.05 for the rejection of the null hypothesis) and with degree of freedom = 1. According to the formula below, the number of failures is "a" – which denotes the failure in transitioning from the absence of difference in the intensities of sweating between the two sides, into the presence of difference in the intensity of sweating between the two sides – and the number of successes is "d" – which denotes the absence of asymmetry in the intensity of sweating between the sides, meaning the sweating in the two sides are equal:
Q2 = (|a-d| 1)2 / a+d
The analysis was performed aiming at comparing the statistical evidence – if they existed at all – for the difference in the ratings attributed to the intensity of sweating between the sides after 1 year of follow-up. The study's null hypothesis (Ho) was "both procedures lead to the same outcome".
Description of the procedures
Right axilla: Liposuction
• Tumescent solution anesthesia is performed with the injection of 250ml 9% saline solution, 10 mL 1% lidocaine injectable solution without vasoconstrictor, 2.5ml 8.4% sodium bicarbonate, and 0.25 ml 1:1000 adrenalin.
• Liposuction is performed with a 2.5mm gauge, two-hole cannula, with the lumen facing up.
Left axilla: Laserlipolysis
• Tumescent solution anesthesia is carried out with the injection of 250ml 9% saline solution, 10 mL 1% lidocaine injectable solution without vasoconstrictor, 2.5ml 8.4% sodium bicarbonate, and 0.25 ml 1:1000 adrenalin.
• Laserlipolysis is performed with the Delight® device (Industra Technologies, São Paulo, Brasil), with 6,000 J of accumulated energy, set on continuous mode, potency at 6W, using the 915nm wavelength. Aspiration was not performed after the laser was applied .
Twelve patients (8 men, 4 women) with primary axillary hyperhidrosis who underwent previous treatment with antiperspirants or topical botulinum toxin type A injection were selected. The mean age was 24 years (min = 17, max = 39) with a mean of 22 years.
The indices of patient satisfaction with the outcomes of the procedures carried out can be seen in Table 1. Seven days after the procedure, 41.6% of the patients described absence of change in the amount of sweating, while 58.4% reported some degree of improvement. Thirty days after all patients described some degree improvement, with 83.3% reporting being completely satisfied. At the end of 1 year of follow-up, the satisfaction index remained positive in all patients, with 75% reporting maximum satisfaction.
An individual patient self-assessment questionnaire and the starch-iodine test were applied, aimed at studying the differences between the outcomes obtained with each of the procedures performed. The self-assessment results are shown in Table 2. After 1 week, 66.6% described the presence of differences between the sides, with 62.5% reporting a greater decrease in sweating on the left. After 30 days, 91.6% of the study patients reported a similar decrease in sweating in the two sides. After 1 year of follow up, 25% reported the presence of differences between the sides, with the right presenting the best results.
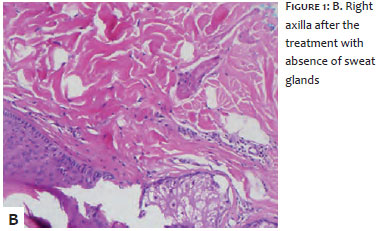
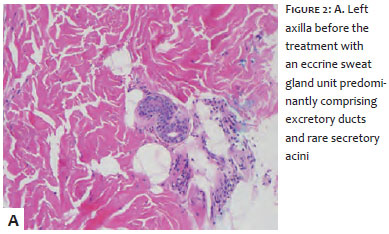
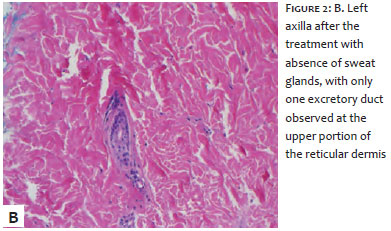
The starch-iodine test evidenced a decrease in sweating in all cases, both at 30 days and after 1 year of follow-up (Table 3). At 30 days, only one case presented differences between the sides, with the right showing a greater decrease in sweating. At 1 year, three patients showed differences between the sides, with the right presenting greater decrease in sweating. The McNemar test with continuity correction for assessing the difference in the intensity of sweating between the two sides was of 1,333, with p = 0.2482. For a p-value greater than a (significance level) Ho is accepted and H1, rejected. As a result, there is no significant difference between the two procedure types regarding the cause and effect of the difference in the results obtained for the intensity in sweating. The histologies performed before and 30 days after the procedure showed absence or decrease of the secretory ducts and acini on both sides (Figure 1A and 1B: right axilla, 2A and 2B: left axilla).
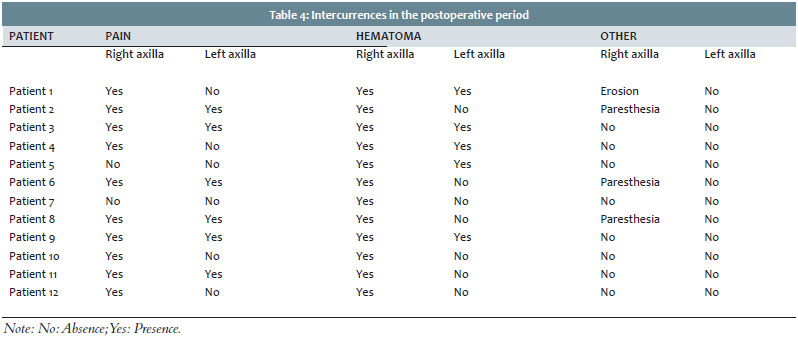
There was absence of intercurrences during the procedures. Postoperative intercurrences can be seen in Table 4. Four patients experienced pain only on the right side, 6 had pain in both sides and none reported pain only on the left side, with a maximum duration of 10 days, being well controlled with ketorolac trometamol. Local hematoma was observed on the right side in all cases, and in the left side in 5 cases. Regression took place in up to 10 days, with the use of a gel containing allantoin and sodium heparin. Temporary paresthesia was reported on the right side in 3 cases, with improvement of symptoms in roughly 90 days with prednisone and Vitamin B1. Skin erosion was reported only in 1 case, in the right side, with improvement in 30 days using silicone gel.
Primary axillary hyperhidrosis affects about 3% of the population in the USA and implies significant emotional and psychosocial consequences. Unlike secondary hyperhidrosis, PAH is not associated with any identifiable underlying condition. 1,3 The limited understanding about the precise pathophysiological mechanism means that its treatment is varied, with varying responses for each therapeutic modality. 2 The present study evaluated the liposuction of eccrine glands, comparing it with 915nm diode laser assisted axillary laserlipolysis. 6
The starch-iodine test demonstrated the presence of decreased sweating in all cases, both at 30 days and after 1 year of follow-up. The histological studies performed before the procedure and 30 days after showed absence or decrease of secretory ducts and acini in both sides. These outcomes are in line with the literature. Leclere 7 described reduced sweating in all evaluated therapeutic modalities, demonstrated by the decrease in the dark areas in the starch-iodine test in all studied groups: 975nm diode laser, association of 924/975nm lasers, isolated curettage, and curettage combined with the association of 924/975nm lasers. That article concluded that the group that underwent last treatment modality had a more significant decrease in sweating. 7
Due to the emission of light beams from diode or 1.064nm Nd:YAG lasers, laserlipolysis generates heat in the axillary region, destroying the glands that produce sweat, promptly and conclusively interrupting its production. 1.6 Laserlipolysis' safety and effectiveness are recognized in the reviewed literature. 6,8 Caplin 8 demonstrated the 1.064nm Nd:YAG laser's efficacy using the starch-iodine test and patient satisfaction scales after 1 year of follow-up. He concluded that it is an effective therapy, with lower levels of adverse effects, 8 a finding that was also observed in the present study.
This study evidenced satisfactory outcomes during the 1 year follow up after the performances of liposuction and laserlipolysis procedures for the treatment of axillary hyperhidrosis refractory to clinical treatment with antiperspirants and botulinum toxin type A. Both techniques showed similar effectiveness at the end of the case's follow up, nevertheless axillary laserlipolysis can be considered a good alternative in the treatment of axillary hyperhidrosis due to the lower frequency of post-operative complications associated to it in the present study. Yet, further studies and more comprehensive patient follow-ups are required in order to confirm this paper's conclusions.
1. Singh S, Davis H, Wilson P. Axillary hyperhidrosis: A review of the extent of the problem and treatment modalities. Surgeon. 2015;13(5):279-85.
2. Stashak AB, Brewer JD. Management of hyperhidrosis. Clin Cosmet Investig Dermatol. 2014 Oct 29;7:285-99.
3. Laser Therapy for Hyperhidrosis: A Review of the Clinical Effectiveness and Guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2015. 19 p.
4. Mordon SR, Trelles MA, Leclere FM, Betrouni N. New treatment techniques for axillary hyperhidrosis. J Cosmet Laser Ther. 2016;16(5):230-5.
5. Lee SJ, Chang KY, Suh DH, Song KY, Ryu HJ. The efficacy of a microwave device for treating axillary hyperhidrosis and osmidrosis in Asians: a preliminar study. J Cosmet Laser Ther. 2013;15(5):255-9.
6. Brown AL1, Gordon J, Hill S. Hyperhidrosis: review of recent advances and new therapeutic options for primary hyperhidrosis. Curr Opin Pediatr. 2014;26(4):460-5.
7. Leclère FM, Moreno-Moraga J, Alcolea JM, Vogt PM, Royo J, Cornejo P, et al. Efficacy and safety of laser therapy on axillary hyperhidrosis after one year follow-up: a randomized blinded controlled trial. Lasers Surg Med. 2015 Feb;47(2):173-9.
8. Caplin D, Austin J. Clinical evaluation and quantitative analysis of axillary hyperhidrosis treated with a unique targeted laser energy delivery method with 1-year follow up. J Drugs Dermatol. 2014;13(4):449-56.
This study was performed at a private practice in São José do Rio Preto (SP), Brazil
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}