


Gerson Dellatorre1; Fernando Eibs Cafrune2
The evolution in surgical techniques for treatment of vitiligo has been producing extremely satisfying results in patients with stable vitiligo, without Köebner phenomenon and resistants to other types of treatment. Many techniques are available and should be used accordingly to the patient and to the dermatologist experience to optimize the results.
Keywords: VITILIGO, SURGERY, TRANSPLANTATION, DERMATOLOGIC SURGICAL PROCEDURES
Melanocytes transplantation procedures are therapeutic options indicated for patients bearing vitiligo in its stable phase and that has not responded to previous clinical treatments. 1 These techniques can potentially yield excellent results, even in anatomical areas that are traditionally refractory, such as distal extremities, elbows, knees, nipple areolas, eyelids and lips. 2 In recent decades, research on surgical treatment of vitiligo has increased substantially, and autologous melanocytes transplantations have become increasingly accessible to dermatologist physicians.
The disease's stability is the most important prerequisite for a successful surgical procedure. 1.3 Most authors define the stability criterion as the absence of new lesions or enlargement of pre-existing lesions within one year. 1,3,4 In cases of doubtful stability, a test can be carried out with the transplantation of four or five mini-grafts using 1.0 mm to 1.2 mm punches in the area to be treated, evaluating whether after a period of three to four months some repigmentation halo has been formed in the region. 5 Absence of the Köebner's phenomenon in candidates to undergo surgery also is of utmost importance, since the surgical manipulation of donor and receptor areas can induce new achromatic lesions. 1 Although it is possible to treat all types of vitiligo with good efficacy using this method, segmental vitiligo tends to yield a better response. 6 Therefore, accurate classification of the disease it is crucial, since it may influence the patient's prognosis.
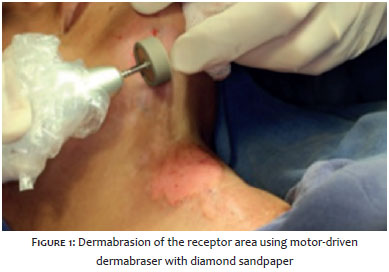
Surgical modalities can to be classified into tissular or cellular techniques, according to the type of graft to be transplanted. 1.4 Most of the techniques require de-epithelization of the receptor area in order it can receive the tissular or cellular graft. This preparation is usually performed applying superficial dermabrasion, which is a simple, widely used and cost effective technique (Figure 1). Other options include the use of carbon dioxide and Er:YAG lasers, suction blisters, curettage and cryotherapy. 7.8
In general, dressings are applied immediately after autologous transplantation surgery, and are left untouched in the treatment area over a period ranging from 7 to 14 days. Their function is to accelerate the healing of the dermabraded areas, prevent bacterial contamination, and keep transplanted tissues or cells in the receptor area. 8 To this end, it is common to use collagen-based and/or non-adherent dressings.
As a complement to the surgical treatment, phototherapy can be performed aimed at increasing the repigmentation outcome. It has been recently demonstrated that the use of narrowband UVB phototherapy in the pre and postoperative periods is related to better repigmentation rates. 9
Punch grafts
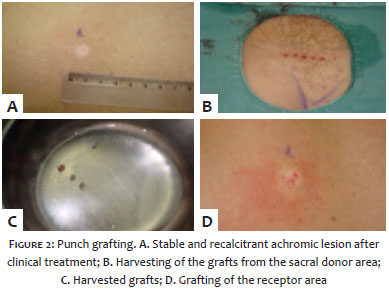
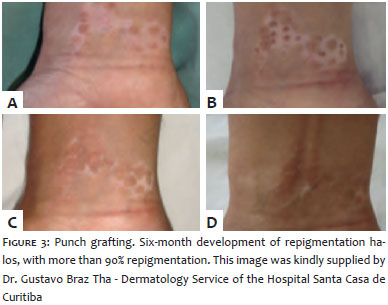
Punch grafting (PG) is a simple, low cost, and widely used technique for the surgical treatment of vitiligo. It consists in obtaining multiple circular grafts from the donor area, taken with 3 mm punches, for subsequent transplantation to the receptor area, which in turn is prepared with punches of the same size (or slightly smaller), in a layout whose spacing corresponds to 2,5x the size of the graft (Figures 2 and 3). 10-12 As an adverse effect, the technique can produce undesirable cosmetic effects known as "cobblestone " appearance, meaning that the graft becomes slightly more elevated than the neighboring receptor area. This is mainly observed when grafts with greater diameters are used. This effect can resolve spontaneously or be treated using electrofulguration. 13 Due to the long time needed to obtain grafts, PG is typically reserved for the treatment of small areas. However, the use of devices with motor driven punchs can reduce this time, allowing the treatment of greater areas. 10
Regarding its effectiveness, a study that included 880 patients showed that 90-100% repigmentation was achieved in 74.55% of patients during a two-year follow-up period. 11
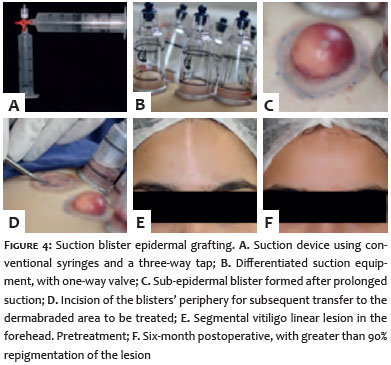
This procedure involves the induction of subepidermal suction blisters in the donor area (usually thighs or arms) by prolonged application of vacuum, with the subsequent transplantation of its roof ? to the receptor area. 1 The vacuum is normally applied with the aid of a syringe or a device specifically used for this purpose (Figure 4). This technique has some advantages over PG, since the donor area heals leaving only a minimal post-inflammatory hyperpigmentation. 14 Moreover, the "cobblestone" effect described for the previous technique does not occur due to the fact that the graft is purely epidermal. 15
According to a recent study, suction blister based epidermal grafting (SBEG) can yield results that vary from good to excellent (65-100% repigmentation) in 80% of patients. Although it is cost effective, this method is deemed as protracted, since approximately two hours are necessary to obtain a blister using a 10ml syringe. That time can be shortened using the anesthetic injections in the dermis or applying heat to the donor area before the blister is obtained. 15.16
Partial thickness skin grafts (PSG) have the advantage of treating large areas with good response (90-100% repigmentation) on a single procedure. The graft is obtained with the assistance of a dermatome, meaning the surgeon must have the proper expertise and experience to conduct the procedure. 17 Furthermore, color incompatibility in the receptor area and the potential for unaesthetic healing in the donor area are possible side effects of this technique. 4
Different melanocyte transplantation techniques have been described using tissue fragmentation. A common characteristic to these techniques is the fact that the harvesting process of the tissue from the donor area leaves the skin macerated into small fragments to be grafted in the receptor area. In general, they are rapid and technically easy to perform methods, and can be carried out in simple and inexpensive surgical settings. They are capable of re-pigmenting areas that are four to ten times larger than the donor area. 18.19
The epidermal curettage (EC) technique is performed after asepsis and demarcation of the donor area (usually thigh or sacral region), where topical or injectable anesthesia is performed. With a sterile curette, the tissue is removed up until the pinpoint bleeding is visualized. The removed material is placed in a jar with saline solution, and may undergo further maceration up until a paste consistency is obtained. After dermabrasion of the receptor area, the macerated tissue is put in place observing a homogeneous distribution. Next, the area is covered with non-adherent dressing. The dressing should be kept in place with restriction of movement for one week. 18 This method leads to rapid re-epithelialization, usually without residual scarring in the donor area.
In the tissular maceration (TM) method, a thin layer of skin (with little dermis) is removed from the donor area with the aid of a flexible blade. The tissue is placed in saline solution and shredded with the aid of a delicate scissors up until the fragments are substantially reduced in size. Once the material has been prepared, it is placed on the dermabraded area, followed by a dressing, just as described in the previous method. 19,20 Absence of scars in the donor area and intense repigmentation (over 90%) were observed in a study. 19
Suspension of non-cultured epidermal cells
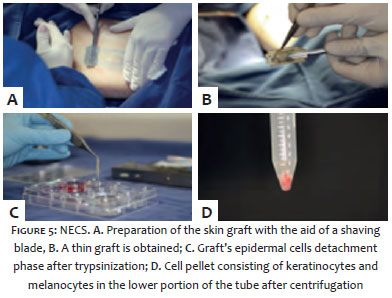
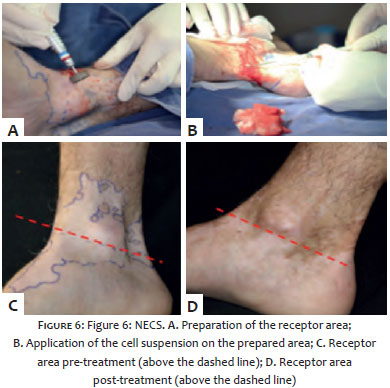
In the non-cultured epidermal cells suspension (NECS), a thin partial thickness graft is obtained from the donor area with the aid of a razor blade or a dermatome (Figures 5A and 5B). Then the tissue fragment is incubated at 37°C in a solution of trypsin with ethylene dinitrilotetrascetic acid (EDTA), which separates the epidermis from the dermis and ungroups the epidermal cells. After centrifugation of the solution, a concentrated suspension of melanocytes and keratinocytes is obtained, re-suspended in a small volume, and transferred to the dermabraded receptor area (Figures 5C, 5D and 6).
This method has the advantage of the possibility of expanding the ration between the donor and receptor areas from five to ten times, meaning it is capable of treating large areas with satisfactory results. 1.4 Good to excellent results (75-100% repigmentation) can be achieved in 89% of patients. 21 Among this technique's disadvantages is the need for expertise and experience for obtaining the donor tissue fragment, in addition to requiring specific laboratory equipment for the trypsinization phase. 1
Suspension of non-cultured cells from the external follicular sheath
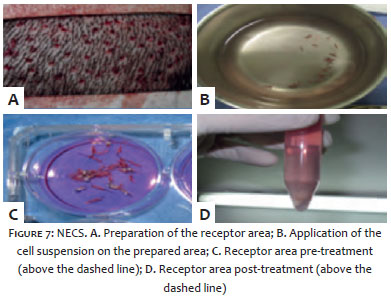
In this procedure, a cellular suspension is obtained from hair follicles obtained using a follicle unit extraction method assisted by small punches - similar to how hairs are obtained in the hair transplant technique (Figure 7). Approximately 15 to 25 follicles are extracted per patient, depending on the area to be transplanted. Once extracted, the hair follicles are subjected to a trypsinization process similar to that of NECS, aiming at obtaining the cellular suspension. 22.23
Obtaining cells originated from hair follicles has some advantages. In addition to being considered an important reservoir region of melanocytes and their precursors, the scars resulting from follicular extraction are virtually invisible. 22 In a comparative and randomized study contrasting NECS and the suspension of non-cultured cells from the external follicular sheath (SNCEFS) conducted with 30 patients, repigmentation of 92% and 78% of the lesions were obtained, respectively. However the difference was not statistically significant. 24
Suspension of cultured cells
The in vitro culture of melanocytes (Figure 8), combined or not with keratinocytes, can dramatically increase the number of transplanted cells. One of the greatest advantages of this technique dwells in the fact that, from a small skin fragment, it is possible to obtain sufficient cells to treat large areas. 25 This method can lead to even greater repigmentation rates when compared to techniques without culture of cells. 25,26 In a recent study, the suspension of cultured cells (SCC) was able to produce more than 90% of re-pigmentation in up to 81.3% of patients. 9
Despite these advantages, the high cost, the dependence on a specialized team and on laboratory cell culture equipment are important disadvantages of the method. 1 Moreover, since the culture media contain mitogenic factors, prolonged follow-up of patients is recommended due to the theoretical potential post-transplantation malignant transformation. 26 Although in some countries this risk is still considered an ethic barrier for the use of the technique for therapeutic purposes, there are an increasing number of studies in the medical literature with absence of adverse events. 9.25
1. Gupta S, Olsson MJ, Kanwar AJ, Ortonne JP, editors. Surgical management of vitiligo. Oxford: Blackwell Publishing; 2007.
2. Mulekar SV, Al Issa A, Al Eisa A. Treatment of vitiligo on difficult-to-treat sites using autologous noncultured cellular grafting. Dermatol Surg. 2009;35(1):66-71.
3. Sahni K, Parsad D. Stability in Vitiligo: Is there a Perfect Way to Predict it? J Cutan Aesthet Surg. 2013;6(2):75-82.
4. Parsad D, Gupta S, IADVL Dermatosurgery Task Force. Standard guidelines of care for vitiligo surgery. Indian J Dermatol Venereol Leprol. 2008; Suppl 74:S37-45.
5. Falabella R, Arrunategui A, Barona MI, Alzate A. The minigrafting test for vitiligo: detection of stable lesions for melanocyte transplantation. J Am Acad of Dermatol. 1995;32(2 Pt 1):228-32.
6. Falabella R. The minigrafting test for vitiligo: Validation of a predicting tool. J Am Acad of Dermatol. 2004;51(4):672-3.
7. Silpa-Archa N, Griffith JL, Williams M, Lim HW, Hamzavi IH. Prospective comparison of recipient-site preparation with fractional carbon dioxide laser vs. dermabrasion and recipient-site dressing composition in melanocyte- keratinocyte transplantation procedure in vitiligo: a preliminary study. B J Dermatol. 2016;174(4):895-7.
8. Al-Hadidi N, Griffith JL, Al-Jamal MS, Hamzavi I. Role of recipient-site preparation techniques and post-operative wound dressing in the surgical management of vitiligo. J of Cutaneous Aesthetic Surg. 2015;8(2):79-87.
9. Zhang DM, Hong WS, Fu LF, Wei XD, Xu AE. A randomized controlled study of the effects of different modalities of narrow-band ultraviolet B therapy on the outcome of cultured autologous melanocytes transplantation in treating vitiligo. Dermatol Surg. 2014;40(4):420-6.
10. Chandrashekar B, Madura C, Varsha D. Autologous mini punch grafting: an experience of using motorized power punch in 10 patients. J Cutan Aesthet Surgery. 2014;7(1):42-5.
11. Malakar S, Dhar S. Treatment of stable and recalcitrant vitiligo by autologous miniature punch grafting: a prospective study of 1,000 patients. Dermatology. 1999;198(2):133-9.
12. Saldanha KD, Machado Filho CD, Paschoal FM. Action of topical mometasone on the pigmented halos of micrografting in patients with vitiligo. An Bras Dermatol. 2012;87(5):685-90.
13. Falabella R. Surgical treatment of vitiligo: why, when and how. J Eur Acad Dermatol Venereol. 2003;17(5):518-20.
14. Ashique KT, Kaliyadan F. Long-Term Follow-up and Donor Site Changes Evaluation in Suction Blister Epidermal Grafting Done for Stable Vitiligo: A Retrospective Study. Indian J Dermatol. 2015;60(4):369-72.
15. Gou D, Currimbhoy S, Pandya AG. Suction blister grafting for vitiligo: efficacy and clinical predictive factors. Dermatol Surg. 2015;41(5):633-9.
16. Kim T, Roh HJ, Kim JY, Noh S, Oh SH. Rapid formation of suction blister through intradermal injection of local anesthetics in epidermal graft for vitiligo. Dermatol Surgery. 2010;36(10):1642-3.
17. Agrawal K, Agrawal A. Vitiligo: repigmentation with dermabrasion and thin split-thickness skin graft. Dermatol Surg. 1995;21(4):295-300.
18. Machado Filho CD, Timoner FR. Epidermal curettage technique (ECT) for tissue harvest from the donor area for melanocyte autologous grafting in cases of vitiligo. An Bras de Dermatol. 2014;89(4):681-3.
19. Krishnan A, Kar S. Smashed skin grafting or smash grafting - a novel method of vitiligo surgery. Int J Dermatol. 2012;51(10):1242-7.
20. 20. Pahwa M, Gupta S, Khunger N. Multimodal single-step vitiligo surgery: a novel approach. Dermatol Surg. 2010;36(10):1627-31.
21. Budania A, Parsad D, Kanwar AJ, Dogra S. Comparison between autologous noncultured epidermal cell suspension and suction blister epidermal grafting in stable vitiligo: a randomized study. B J Dermatol. 2012;167(6):1295-301.
22. Vinay K, Dogra S, Parsad D, Kanwar AJ, Kumar R, Minz RW, et al. Clinical and treatment characteristics determining therapeutic outcome in patients undergoing autologous non-cultured outer root sheath hair follicle cell suspension for treatment of stable vitiligo. J Eur Acad of Dermatol Venereol. 2015;29(1):31-7.
23. Kumar A, Mohanty S, Sahni K, Kumar R, Gupta S. Extracted hair follicle outer root sheath cell suspension for pigment cell restoration in vitiligo. J Cutan Aesthet Surg. 2013;6(2):121-5.
24. Singh C, Parsad D, Kanwar AJ, Dogra S, Kumar R. Comparison between autologous noncultured extracted hair follicle outer root sheath cell suspension and autologous noncultured epidermal cell suspension in the treatment of stable vitiligo: a randomized study. B J Dermatol. 2013;169(2):287-93.
25. Chen YF, Yang PY, Hu DN, Kuo FS, Hung CS, Hung CM. Treatment of vitiligo by transplantation of cultured pure melanocyte suspension: analysis of 120 cases. J Am Acad Dermatol. 2004;51(1):68-74.
26. Verma G, Varkhande SR, Kar HK, Rani R. Evaluation of repigmentation with cultured melanocyte transplantation (CMT) compared with non-cultured epidermal cell transplantation in vitiligo at 12th week reveals better repigmentation with CMT. J Invest Dermatol. 2015;135(10):2533-5.
This study was performed at the Hospital Santa Casa de Curitiba - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}