


Gerson Dellatorre
Dear Sirs,
In recent years, surgical treatment of vitiligo has been an area of great academic interest for us. We were enthused with the recent paper entitled Grafting by epidermal scraping in stable vitiligo: a therapeutic option (DOI: http://dx.doi.org/10.5935/scd1984-8773.201682760),1 for it addresses a therapeutic modality – melanocyte transplantation – which is still little used in Brazil. However, we have noticed that readers could misinterpret some of the remarks made in literature review carried out by the authors. In this manner, we would like to address those remarks in a critical and constructive way.
In the article's abstract and introduction, the authors state that surgical treatment of vitiligo is preferred over clinical treatment in case of disease stability. However, the idea that surgical treatment should be applied only in cases that are refractory to clinical treatment (besides being stable and devoid of the Köebner's phenomenon) still predominates in practice and literature, as can be verified in seminal articles on the subject.2-4 Based on this fact, we deem that in light of the risks inherent in any surgical procedure (albeit minimal in this context), clinical treatment should still be tried in the first instance, even in cases of stable vitiligo and devoid of Koebner's phenomenon.
In the Discussion section, first paragraph, where it reads "The main advantage of this method as compared to the original punch micrografting technique is that it does not lead to the "cobblestone" aspect in the treated area, dyschromias in the donor and recipient areas, (...)", we find it difficult to state so categorically that the technique does not lead to dyschromia in the recipient and donor areas. In principle, any surgical technique for transplantation of melanocytes can lead to that condition. The presence of dyschromia (hyperchromia in both the donor and the recipient areas) is seen in the surgical outcome of the paper in question. Although they are often temporary, dyschromias can remain indefinitely, regardless of the technique used. I would like to point out that even more "conservative" techniques for obtaining the tissue, such as Suction Blister Epidermal Grafts (SBEG) method, can leave residual hyperchromia in around 40% of cases, as reported in a recent study.5
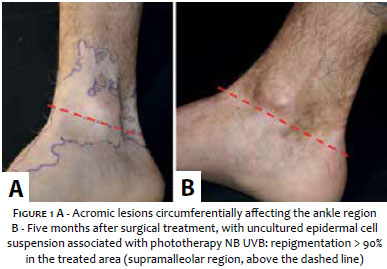
Regarding the statement "The acral regions and the areas over the joints should be avoided – especially in very young patients – for it is considerably difficult to implement the techniques in these locations and there is risk of treatment failure", it is important to note that assuming that the primary indications for the surgical treatment of vitiligo (stable disease, absence of Köebner phenomenon and refractoriness to clinical treatment) are fulfilled, these areas can be treated with surgical technique. Although repigmentation rates are lower than those provided by surgical treatment in other areas – such as the face, for example – the technique still achieves good results in more than 50% of cases, as has already been demonstrated in the literature.6 A recent example is the case of a young patient with vitiligo circumferentially affecting the ankle region, which was successfully treated by us using the uncultured epidermal cell suspension technique (Figure 1).
Moreover, the technique is also not contraindicated for lips and eyelids, as set out in Table 1 of the article in question.1 On the contrary, it is often used for this purpose.4
Furthermore, we consider that the contraindication for young patients is only subjective. In fact, it depends on the patient's understanding and collaboration during the operative and postoperative periods (period during which the dressing must be in place). Studies have already shown the method's safety in this age group, with good therapeutic outcomes.7
Finally, contrary to what was reported in Table 1 of the article in question, surgical results with cultured melanocytes suspension are already well reported in the literature, with more than 400 cases treated only in the study conducted by Zhang et al.8
1. Elias BLF, Ferreira FR, Lima EMA, Amarante CF, Mandelbaum SH. Enxerto por raspagem epidérmica no vitiligo estável: uma opção terapêutica. Surg Cosmet Dermatol. 2016;8(2):173-7.
2. Parsad D, Gupta S, Force IDT. Standard guidelines of care for vitiligo surgery. Indian journal of dermatology, venereology and leprology. 2008;74 (Suppl):S37-45.
3. Falabella R. Surgical treatment of vitiligo: why, when and how. Journal of the European Academy of Dermatology and Venereology: J Eur Acad Dermatol Venereol. 2003;17(5):518-20.
4. Paul M. Autologous Non-cultured Basal Cell-Enriched Epidermal Cell Suspension Transplantation in Vitiligo: Indian Experience. J Cutan Aesthet Surg. 2011;4(1):23-8.
5. Ashique KT, Kaliyadan F. Long-Term Follow-up and Donor Site Changes Evaluation in Suction Blister Epidermal Grafting Done for Stable Vitiligo: A Retrospective Study. Indian J Dermatol. 2015;60(4):369-72.
6. Mulekar SV, Al Issa A, Al Eisa A. Treatment of vitiligo on difficult-to-treat sites using autologous noncultured cellular grafting. Dermatol Surg. 2009;35(1):66-71.
7. Sahni K, Parsad D, Kanwar AJ. Noncultured epidermal suspension transplantation for the treatment of stable vitiligo in children and adolescents. Clin Exp Dermatol. 2011;36(6):607-12.
8. Zhang DM, Hong WS, Fu LF, Wei XD, Xu AE. A randomized controlled study of the effects of different modalities of narrow-band ultraviolet B therapy on the outcome of cultured autologous melanocytes transplantation in treating vitiligo. Dermatol Surg. 2014;40(4):420-6.
The present study was performed at the author's private practice - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}