


Célia Luiza Petersen Vitelo Kalil1; Stela Cignachi2
Keloids have functional, aesthetic and psychological impacts that can influence the patients' quality of life. Moreover, given the high rate of recurrence – particularly in large lesions located in the anterior thoracic region – they are more difficult to treat. This paper reports a successful treatment for keloids in this area using a new technique that combines intense pulsed light, botulinum toxin type A and the conventional treatment with injection of corticosteroids.
Keywords: KELOID; INTENSE PULSED LIGHT THERAPY; BOTULINUM TOXINS, TYPE A; ADRENAL CORTEX HORMONE
Keloids are benign lesions consisting of the exuberant hyperplasia of the dermis' differentiated connective tissue. It can arise from changes in the skin healing process or be induced by trauma caused by lacerations, tattoos, burns, injections, bites and vaccines, as well as dermatoses, such as acne.1
This type of scarring can occur in various body regions, preferably in sites above the abdomen, such as the thorax, shoulders and neck. Some related symptoms, such as pruritus, pain and restricted mobility, collaborate to the worsening of the affected patients' quality of life.1
This type of scar formation's exact pathophysiology is unknown,2 although several studies have demonstrated high levels of transforming growth factor beta (TGFb1) in the keloids' fibroblasts, including increased collagen production and integrin expression, decreased expression of metalloproteinases and of inhibitors of metalloproteinases. 3
Many treatments are available, however most of them have constraints and limited resolution.4 Some of the established treatments, such as intralesional corticosteroids and silicone plates, are used to treat unsightly scars due to their ease of use. In patients with wide scars, where the difficulty of treatment is even greater, surgical removal is usually employed.3 Other types of treatment combining techniques have been described, and among them are adjuvant radiotherapy, intralesional injections of 5-fluourouracil or bleomycin, interferon or imiquimod applications and betatherapy.1
Nevertheless, the improvement of the appearance of the lesion by more than 80% is rare in light of the need for maintaining the treatment and the difficulties arising from the dimensions and location of the lesions.4 Aiming at decreasing such limitations and achieving better outcomes, the authors propose a new treatment modality based on the triple therapy using intralesional corticosteroids, intense pulsed light (IPL) and botulinum toxin type A (BTXA).
A 25 year-old female patient, Fitzpatrick phototype II, born and raised in the city of Canoas, in the Southern Brazilian State of Rio Grande do Sul, with a family history of keloids sought treatment for a single cicatricial keloid lesion with irregular borders, erythematous in color, painful to palpation, located in the central region of the anterior chest wall, measuring 8 x 1.7cm, with progressive growth for the previous 15 years. She reported the onset of the lesion following a viral disease, describing various unsuccessful treatments with cryotherapy and corticosteroids (Figure 1).
The patient underwent the application of occlusive topical anesthetic with 10% lidocaine and 7% tetracaine for 40 minutes in the keloid area, followed by local antisepsis with 2% aqueous chlorhexidine. The triple therapy combined treatment was carried out with four monthly sessions, according to the following sequence:
1) 540nm IPL, 12mm tip, 15ms pulse duration, 15-17 J/cm2 fluence range, 1-2 passes, cooling 5, across the lesion. The device used was the IPL ETHEREA® (INDUSTRA® Technologies, São Paulo, Brazil).
2) 28UI Onabotulinumtoxin A (Botox®) 100 IU vial, 2.5ml dilution in 0.9% saline solution, applied uniformly in the subdermal plane.
3) 1ml intralesional corticosteroid, 40mg/ml. The application was performed in an evenly fractionated way: the drug was applied across the keloid. The area with greater hypertrophy received a greater amount of the substance.
After the procedure, the treated area was occluded with micropore. The patient was instructed to remove it after 24 hours, maintaining the occlusion of the area treated with a silicone plate at night and using sunscreens during the day.
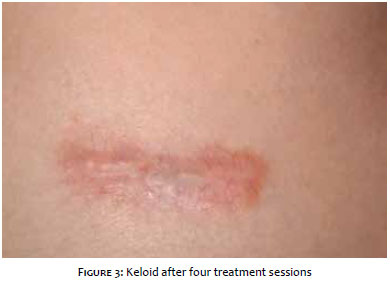
There was improvement in the lesion's thickness in all treated areas – more markedly in the more elevated portions, improvement of the erythema and decreased local vascularization. The patient had clinical improvement of the pain and discomfort, as well as a reduction in the growth of the lesion since the beginning of treatment, showing satisfaction with the outcomes (Figures 2 and 3).
Keloids are pathological scars known as fibroproliferative, thick and elevated alterations that extend laterally to the initial margins of the skin's lesion, being primarily characterized by the overproduction of collagen fibers and secondarily by the hyperplasia of fibroblasts.5 They do not regress spontaneously and have a tendency to recur after resection. Additionally, keloids are not aesthetically acceptable, especially if associated to symptoms. Currently, there is no universally accepted isolated therapy or combination of techniques that allow an effective treatment and prevent recurrence.
The present case report describes a keloid lesion in active and symptomatic phase, located in an anatomical region of difficult control, therefore offering greater difficulty for achieving satisfactory outcomes using conventional treatments. As a result, the authors chose the combined treatment with IPL, BTXA and injection with corticoid, already described by Wu.6
Studies have recently shown the importance of the combination of techniques – such as surgery, laser and drugs – for achieving better outcomes in the treatment of unsightly scars,7 introducing algorithms for the treatment of scars based on the type of cicatricial lesion.
Few studies have reported the IPL effectiveness in the treatment of hypertrophic scars or keloids, quoting limitations in the use of this type of treatment for high phototypes, due to the risk of pigmentary complications.1 Some have shown improvement in reducing the texture, size and color of the treated keloid, while another suggests the need for at least six sessions at intervals of two to four weeks so that there is improvement regarding the reduction of size in the hypertrophic scar being treated. Using IPL, the authors of the present study obtained improvement in the keloid's vascular appearance, erythema and pain, in addition to a reduction in the size by decreasing the local inflammatory component with only four sessions.
Another technique used in combination included BTXA. Recent studies describe that the use of BTXA as monotherapy assists in inhibiting the growth of hypertrophic scars and improves their appearance by inactivating fibroblasts, and can inhibit the expression and proportion of collagen type I and III.8 Other studies observed improvements in the lesion's volume, and tension, and in the recurrence in two or three-month treatments. Nonetheless, they concluded that the clinical efficacy of BTXA remains unclear.9 Additionally, keloids have a greater density of nerve fibers in the dermis than the normal skin. In addition, these nerve fibers are located in deeper planes. In this manner, it was possible to observe that there was a decrease in the keloid's size and proliferative activity after the inhibition of the nerve impulse transmission via subdermal injections of BTXA, due to the reduced tension of muscle activity between the cicatricial fibers.10
The injection of corticoid was used in combination with IPL and BTXA, determining the inhibition of protein synthesis and fibroblasts migration. In the study carried out by the authors of the present paper, it was possible to observe a significant regression of the patient's symptoms due to the decrease in the lesion's volume component.
After treatment, the authors chose to use a silicone plate for local compression, maintaining the mechanical pressure and leading to the reorganization of collagen fibers during the treatment. Although this mechanism is not completely understood, it is hypothesized that due to the impermeability on the stratum corneum, there is a continuous hydration of the skin, with a reduction in the incipient hyperemia and fibrosis.5
The outcome obtained demonstrates the efficacy of the triple therapy in the treatment of keloids, despite the recurrence rates of active, symptomatic lesions with unfavorable prognostic factors, such as difficult locations. Moreover, it showed that there is an association of the vascular inflammatory activity, neurological stimulation and collagen hyperproliferation in fibroproliferative scarring. The treatment proposed for this keloid – with the combination of techniques – was safe and well tolerated, and should be considered in the management of this type of lesions.
1. De Oliveira Junior B, Lastoria JC, Pereira HR, Silveira LVA, Oliveira LP, Stolf HO. Estudo comparativo entre o tratamento radioterápico com elétrons e betaterapia, após cirurgia de queloides. Surg Cosmet Dermatol. 2009;1(2):53-7.
2. Mamalis AD, Lev-Tov H, Nguyen DH, Jagdeo JR. Laser and light-based treatment of Keloids - a review. J Eur Acad Dermatol Venereol. 2014;28(6):689-99.
3. Li W, Wang Y, Wang X, Liu Z. A Keloid Edge Precut, Preradiotherapy Method in Large Keloid Skin Graft Treatment. Dermatol Surg. 2014;40(1):52-7.
4. Vrijman C, Drooge AM, Limpens J, Bos JL, Van der ven JPW, Spuls PI. Laser and intense pulsed light therapy for the treatment of hypertrophic scars: a systematic review. Br J Dermatol. 2011;165(5):934-42.
5. Berman B, Perez OA, Konda S, Khout BE, Vieira MH, Delgado S. A Review of the Biologic Effects, Clinical Efficacy, and Safety of Silicone Elastomer Sheeting for Hypertrophic and Keloid Scar Treatment and Management. Dermatol Surg. 2007;33(11):1291-302; discussion 1302-3..
6. Wu WTL. Skin resurfacing with microbotox and the treatment of keloids. In: Benedetto AV, editor. Botulinum toxins in clinical aesthetic practice. 2th. New York: Taylor & Francis, 2006. p: 109-205.
7. Waibel JS, Rudnick A. Current trends and future considerations in scar treatment. Semin Cutan Med Surg. 2015;34(1):13-6.
8. Antonio CR, Antônio JR, Trídico LA. Toxina botulínica: revisão de sua aplicabilidade em doenças ao alcance do dermatologista. Surg Cosmet Dermatol. 2014;6(3):268-76.
9. Gauglitz GG. Management of keloids and hypertrophic scars: current and emerging options. Clin Cosmet Investig Dermatol. 2013;6:103-14.
10. Haedersdal M, Moreau KE, Beyer DM. Fractional nonablative 1540 nm laser resurfacing for thermal burn scars: a randomized controlled trial. Lasers Surg Med. 2009;41(3):189-95.
The present study was carried out at the authors' private practices - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}