


Fernanda Freitas de Brito1; Tatiana Cristina Pedro Cordeiro de Andrade2; Letícia Marra da Motta1; Maria Lopes Lamenha Lins Cavalcante1; Cleverson Teixeira Soares3; Sadamitsu Nakandakari3
The Merkel cell carcinoma is a rare and highly aggressive neuroendocrine skin tumor. The purpose of this paper is to warn of the possibility of this diagnosis, usually not considered as an initial hypothesis in cutaneous neoplasias. The authors describe two cases of elderly female patients with complaints of a single erythematous nodule on the face. The diagnoses of basal cell carcinoma and amelanotic melanoma were considered. The presence of telangiectasias was evident at dermoscopy. The incisional biopsy's histology evidenced Merkel cell carcinomas. This neoplasia typically occurs in Caucasian patients with over 65 years of age, emerging as an erythematous-purplish nodule of rapid growth, with immunohistochemistry being essential for the diagnosis.
Keywords: SKIN NEOPLASMS; CARCINOMA, MERKEL CELL; NEUROENDOCRINE TUMORS; IMMUNOHISTOCHEMISTRY
The Merkel cell carcinoma (MCC) – or primary neuroendocrine carcinoma of the skin – was first described by Cyril Toker in 1972.1-3 This is a malignant proliferation of highly anaplastic cells that share characteristics with those derived from the neuroectoderm. The estimated incidence in the United States is 0.32 cases/100,000 people.3 An increase in the number of reported cases has been observed more recently, especially after the emergence of new immunohistochemical markers.2 When conducting diagnoses, physicians rarely suspect of the presence of this lesion. In a study with 106 patients diagnosed with primary MCC, this clinical hypothesis was suggested in only 1% of cases.3 The objective of the present paper is to describe two cases diagnosed at a referral center and raise the alert regarding the possibility of MCC, which is often not considered as an initial hypothesis in cutaneous neoplasias, as well as to highlight the importance of early diagnosis and treatment.
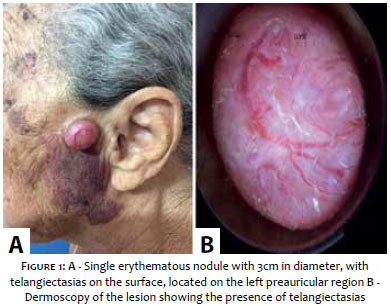
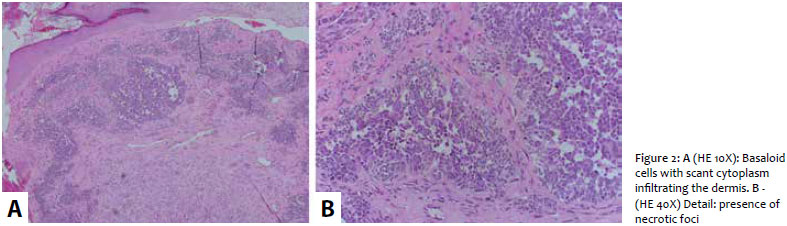
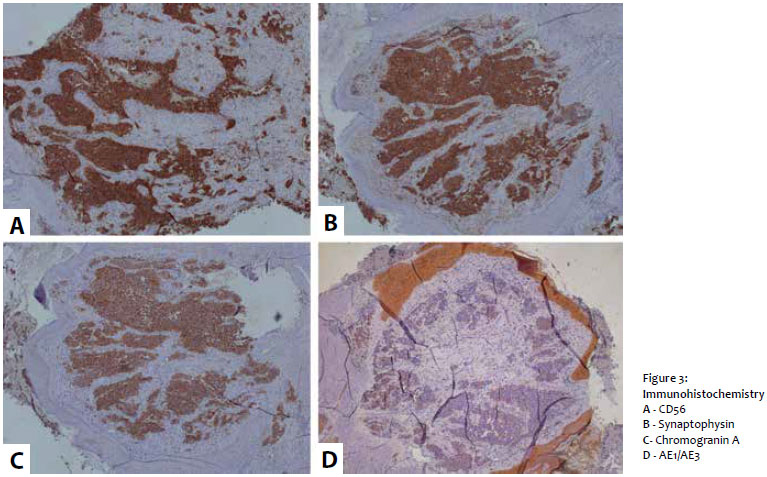
Case 1: A 78 year-old female patient sought medical care complaining of nodular lesions in the left pre-auricular region for roughly two months. Her personal history included systemic hypertension and hypothyroidism. The dermatological examination revealed a single erythematous nodule with 3cm in diameter and telangiectasias on its surface, located on the left preauricular region (Figure 1A). The presence of telangiectasias was evident under dermoscopy (Figure 1B). In light of the clinic history and dermatological examination, the diagnoses of basal cell carcinoma and amelanotic melanoma were hypothesized. An incisional biopsy was then carried out and the material sent for histology and immunohistochemistry. The anatomopathological result evidenced infiltration of basaloid cells, with scant cytoplasm in the dermis (Figure 2A) and presence of necrosis foci (Figure 2B). The immunohistochemistry was positive for cytokeratin 20 (CK20), chromogranin, synaptophysin, CD56 and AE1/AE3 (Figures 3A and B), confirming the diagnosis of Merkel cell neuroendocrine carcinoma.
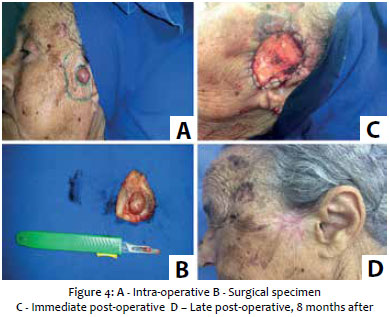
The patient was referred for surgical treatment in the authors' dermatologic service having undergone excision with 3cm margins and continuous suture anchored on the borders with 4.0 nylon for hemostasis (Figures 4A, B and C) and healing by second intention with activated carbon dressing. The patient returned for weekly dressings, with the activated carbon maintained until week 9. Dressings with Kollagenase® (Cristalia Produtos Químicos, São Paulo, Brasil) were applied from week 10 up until the healing was complete (Figure 4D).
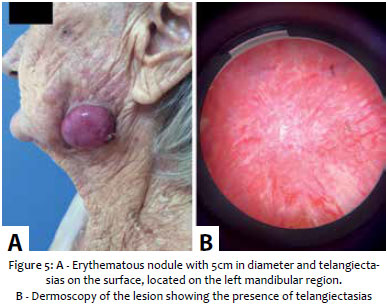
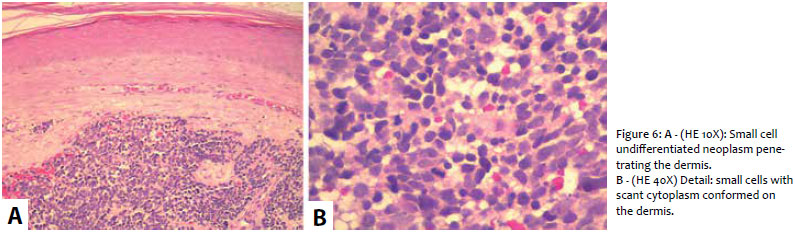
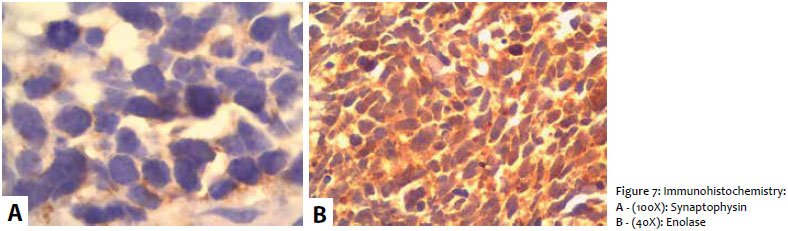
Case 2: An 87 year-old female patient (widow, rural worker) sought medical care complaining of a nodular lesion in the left mandibular region that had emerged five months before and had progressive growth. Personal history included lung disease and current use of aminophylline – she had smoked Brazilian tobacco rolled in corn leaves for 50 years in the past. The dermatological examination revealed a nodule with erythematous, smooth glossy surface in the left mandibular region, with 5cm in diameter and many telangiectasias (on the surface) (Figure 5A). In addition, there was presence of a palpable perilesional, hardened and fixed lymph node. Dermoscopic examination showed the presence of telangiectasias (Figure 5B). In light of the clinical history and dermatologic examination, the hypotheses of Merckel cell carcinoma and amelanotic melanoma were considered. After an incisional biopsy with histologic and immunohistochemical studies, the pathological results showed the presence of a undifferentiated small cell neoplasia penetrating the dermis (Figure 6A), and small cells with scant cytoplasm conformed on the dermis (Figure 6B). The immunohistochemistry was positive for enolase and synaptophysin (Figure 7), confirming the diagnosis of neuroendocrine Merkel cell carcinoma. The patient was referred for surgical treatment at the oncology department due to the presence of palpable satellite lymph node and metastasis to the parotid gland.
The Merkel cell carcinoma is highly aggressive neuroendocrine skin tumor.1,4,5 It typically occurs in Caucasian patients with over 65 years of age, with a slight predominance in men,2,3,5 – which was not observed in the two cases described in the present paper. It manifests clinically as a single painless, erythematous-purplish nodule,4,3,6,7 of rapid growth and aggressive nature.2,5 Telangiectasia are often observed. The most common sites involved are the head and neck (40 - 50%),2 followed by the trunk and limbs. Its etiology remains unclear, and the hypothesis that describes the tumor as originating from Merkel cells – as a mechanoreceptor of the basal layer of the epidermis – or from pluripotent stem cells which later differentiate into neuroendocrine is controversial.2,3,5 In a study with 27 MCC cases, 41% were associated with other epithelial lesions, such as carcinoma in situ squamous cell carcinoma , invasive squamous cell carcinoma, basal cell carcinoma and actinic keratosis.1,3 These findings strengthen the hypothesis of pluripotent stem cell origin in the epidermis, potentiated by the UV radiation's mutagenic effects.3 Other risk factors include: immunosuppression and polyomavirus infection.1,3 Immunohistochemistry is crucial for the differential diagnosis with other tumors.3 There is positivity for epithelial proteins – such as cytokeratins – and neuroendocrine markers – such as neuron-specific enolase, synaptophysin, CD56 and chromogranin A.2,3,6,8 In particular, CK20 is an important marker of MCC, offering high especificity.2 About 5% of patients do not express CK20. Differential diagnosis includes: hemangioma, angiosarcoma, small cell cutaneous lymphoma, non-melanoma skin cancer, amelanotic melanoma, Ewing's sarcoma, cutaneous metastases of pulmonary small cell carcinoma, neuroblastoma and rhabdomyosarcoma.2 Unlike other nonmelanoma skin cancers, MCC has a high propensity to metastasize and regionally and distally.2 Lymph nodal spread occurs early and frequently, with approximately 20% of cases presenting clinically positive lymph nodes.2 The main sites of metastases are the liver, bones, lung, brain and non-regional lymph nodes.2,5,6 Due to the rarity of the tumor, there are few treatment protocols based on evidence, nevertheless surgery and radiotherapy are the main therapies.1 The initial treatment consists of surgical excision with margins in excess of 3cm.2,5,8 The indication of prophylactic lymphadenectomy due to the high probability of lymph node metastasis is debatable since whilst there is a higher locoregional disease control, it does not improve survival.5 Adjuvant radiotherapy is often recommended and is associated with decreased local and locoregional recurrence, and increased survival.2,5 Adjuvant chemotherapy is controversial and its use is limited. 5 Clinical diagnosis of MCC is complex, however suspecting of its presence is important for early diagnosis and treatment,3,5 factors that can have a positive impact on the patient's survival.
1. Saxena A, Rubens M, Ramamoorthy V, Khan H. Risk of Second Cancers in Merkel Cell Carcinoma: A Meta-Analysis of Population Based Cohort Studies. J Skin Cancer. 2014: 1-7.
2. Mello DF, Ricciluca L, Felix M, Rodrigues A, Junior AH. Carcinoma das células de Merkel: relato de 2 casos. Rev Bras Cir Plást. 2010; 25(1): 217-21.
3. Rossoe EWT, Fernandes KKML, Prado IDF, Bazzo ILMS, Tebcherani AJ, Santos TC. Tumor de Merkel: relato de caso. Surg Cosmet Dermatol. 2012; 4(3): 268-70.
4. Priante AVM, Alves FV, Taborda MF, Oliveira, MF. Carcinoma de células de Merkel em pele de face. Rev Bras OncoL Clín. 2012; 8(28): 88-90.
5. Almeida MWR, Lopes CC, Junior HLA, Costa LE. Carcinoma de células de Merkel em extremidade inferior. Rev Col Bras Cir. 2012; 39(2): 165-67.
6. Becker JC. Merkel cell carcinoma. Ann Oncol. 2010; 21(7): 81-5.
7. Marchesi A, Parodi PC, Brioschi M, Sileo G, Marchesi M, Vaienti L. Giant Merkel cell carcinoma of the lower limb: case report and review of the literature. J Cutan Med Surg. 2013;17(5): 351-5.
8. Lien MH, Baldwin BT, Thareja SK, Fenske NA. Merkel Cell Carcinoma: Clinical Characteristics, Markers, Staging and Treatment. J Drugs Dermatol. 2010; 9(7): 779-84.
This study was conducted at Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}