


Luiz Eduardo Garcia Galvão1; Heitor de Sá Gonçalves2; Juliana Chagas Caldas3; Carolina Muratori Cavalcante3
Introduction: Actinic keratoses are the most common premalignant skin lesions, with a chronic and recurrent nature. Daylight photodynamic therapy has been used in the treatment of actinic keratoses of the face and scalp.
Objective: To demonstrate the possibility of implementing daylight photodynamic therapy at a public service, for the treatment of facial actinic keratosis, using one tube of methyl aminolevulinate cream for up to four patients.
Methods: Ten patients were selected to undergo daylight photodynamic therapy at the Centro de Dermatologia Dona Libânia, located in the city of Fortaleza (CE), Brazil. Curettage was performed on the actinic keratosis and a methyl aminolevulinate cream based chemical filter was applied across the face.
Results: One tube of methyl aminolevulinate cream was enough for treating up to four patients with multiple facial actinic keratoses, whereas studies suggest the use of at least one gram to treat one face completely.
Conclusion: It was possible to conclude when administering daylight photodynamic therapy, an amount of less than one gram of methyl aminolevulinate cream in the treatment of facial actinic keratoses is a dosage sufficient to obtain an effective clinical response.
Keywords: KERATOSIS, ACTINIC; PHOTOCHEMOTHERAPY; ECONOMICS, PHARMACEUTICAL
Actinic keratoses (AKs) are the most common premalignant skin lesions, also being chronic and recurrent in character.
They are usually located in sun-exposed areas of the body, such as the scalp, face and forearms, of individuals with fair skin phototypes, who are immunosuppressed, bear some genodermatosis or undergoes chronic exposure to UV radiation.1 Many studies have tried to estimate its true prevalence in the general population, arriving at varied rates, depending on racial factors, age, assessed anatomical site and selection methods used in the analysis. In Australia, currently the country with the highest known rate of AK in the world, 40-50% of individuals over 40 have at least one lesion due to the large proportion of fair phototypes in its population.2 Actinic keratosis can be clinically classified in Grade 1 – when the lesions are slightly palpable, erythematous or rough; Grade 2 – when lesions have the appearance of erythematous desquamative plaques; or Grade 3 – when lesions are hypertrophic.3 Studies describe varying degrees of progression into invasive squamous cell carcinoma (SCC), with about 0.025% to 16% of the AKs undergoing transformation into SCC over the years, with the treatment of all these pre-neoplastic lesions being required.4
Photodynamic therapy (PDT) is the first line treatment for multiple AKs of the face and scalp.5 The concept underpinning PDT in AK is the induction of cytotoxicity in proliferating cells, using a light source with an adequate wavelength. O treatment starts with the application of a solution of 20% 5-aminolevulinic acid (ALA) or 16% methyl aminolevulinate cream (MAL) over an AK area on the face and/or scalp. These are not photosensitizing agents themselves, however they are metabolic precursors of the active compound protoporphyrin IX (PpIX) via the biosynthesis of the intracellular heme.6 Protoporphyrin IX is deemed as a potent photosensitizing agent and is easily photo inactivated, meaning that it is degraded when exposed to a specific source of light. Protoporphyrin IX has several peaks of light absorption, the main one corresponding to the Soret band at 405nm, equivalent to blue light. Other lower peaks are also important and are called Q bands. Although Q bands' peaks are lower than the 405nm peak, many studies regarding PDT are performed using light sources in the red light spectrum between 620nm and 635nm due to the fact that red light provides greater penetration into the tissue, optimizing PDT for deeper lesions.7 After a variable period of contact with the skin – in the case of ALA and three hours under occlusion with plastic film and aluminum foil, in the case of MAL cream, synthesis of PpIX occurs, which in the presence of reactive oxygen and light with the appropriate wavelength, causes necrosis and apoptosis in dysplastic keratinocytes, therefore evidencing the presence of selective action on clinical and subclinical AK.
Recent studies have shown that TFD can be performed with the daylight (PDT- DL).8 In this procedure, PpIX is activated by visible light, which contains the first's two peaks of absorption (blue and red), allowing treatment of AK lesions with less adverse effects of painfulness and erythema. In 2008, Wiegell et al. compared the effects of applying conventional photodynamic therapy (PDT-C) associated with MAL after incubation for 180 minutes with those of PDT-DL during exposure to natural light for 150 minutes, for the treatment of AK in the face and scalp.9 Continuous production of PpIX in PDT-DL during the outdoor exposure period was demonstrated to be as effective as PDT-C, nevertheless with higher tolerance to pain and a less erythema in the post-procedure period.10
The PDT-DL consensus currently indicates that the procedure should be carried out at an outdoor temperature of between 10ºC and 35ºC, avoiding very cloudy or rainy days.11
After preparation of the facial or scalp skin with curettage of the AK lesions, the application of chemical sunscreen – without titanium dioxide or zinc oxide – is performed for protection from UV rays, without prejudice of penetration of visible light, which promotes PpIX synthesis. The absence of the solid physical component in the cream enables the activation of PpIX by visible light while maintaining protection against UV radiation. The application of chemical sunscreen can alternatively be carried out before the preparation of the skin, according to the dermatologist's preference. Next, MAL cream is applied throughout the treated area, and the patient is instructed to begin outdoor exposure within 30 minutes. This exposure should take place in the shade for two hours. Once that time is elapsed, the MAL cream should be removed and the photoprotection care intensified.12
When compared with PDT-C, PDT-DL's has the advantages of increased patient tolerance, minimum local cutaneous reactions and absence of dependence of an artificial light source at the practice. Yet, it is the high cost of the MAL cream that precludes the indication of any type of PDT treatment in public hospitals and private practices that are subjected to unfavorable socio-economic conditions, as is the case, for instance, in Latin America.
The present study was aimed at demonstrating the viability of performing PDT-DL – which is per se more cost effective than PDT-C – in public services to successfully treat facial AK using a single MAL cream tube for 4 patients, depending on the extent of the AK and dimensions of the patient's face.
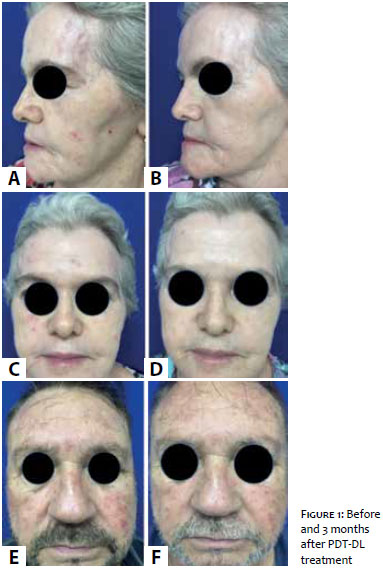
Ten patients were selected in July 2015 to undergo PDT-DL, observing the following inclusion criteria: skin phototypes I-IV, presence of at least four AK lesions on the face, regular use of sunscreen and at least one previous alternative treatment for facial AK (such as cryotherapy and 5-fluorouracil cream) more than six months before taking part in the study. All procedures were performed at Dermatology Center Dona Libânia, in the Brazilian Northeast city of Fortaleza (CE), with outdoor exposure, in the shade, from 7:30AM to 9:30AM, after curettage of the AK and application of chemical filter and MAL cream across the face, including the auricles. Sunscreen was applied in the other sun-exposed body areas, such as neck and arms. All patients were photographed before and three months after the PDT-DL session. The ethical principles emanating from the Helsinki Declaration were followed in the present study.
There was absence of important skin reactions and the patients experienced a reduction in the number of AKs according to clinical and photographic tests performed three months after the PDT-DL procedure (Figure 1 A and B). It was possible to treat 8 female patients and 2 male patients (two albinos) with 3 MAL tubes of 2g each. Of the 3 MAL tubes used, 2 were used to treat 6 patients and 1 was used to treat 4 patients (Figure 1 C, D, E and F).
Daylight photodynamic therapy allows the treatment of large areas of the face and scalp in patients with multiple AKs. In contrast with PDT-C, it is possible to treat the cutaneous cancerization field with less discomfort, for there is continuous production of PpIX during the two hours of outdoor exposure.13 Erythema, edema and desquamation after the session are far less intense when compared to those resulting from the conventional technique and even other treatments conducted at home, such as 5-fluorouracil and imiquimod cream. It is important to observe the weather conditions with a view to a possible rescheduling of the procedure, completely avoiding it if rain or cloudy weather with dark clouds are forecast for the time of the outdoor exposure. The city of Fortaleza is located in the Northeast Brazilian state of Ceara, at a low latitude (03° 43' 02" S), where the average annual temperature is 26.3 °C and the average annual rainfall is 1,448mm (max rainfall in April = 329mm, min rainfall in October = 13mm). These characteristics allow that PDT-DL be performed throughout the year. Other Brazilian cities may have higher rainfall and fewer sunny days, nevertheless as the minimum temperature for the procedure is 10 °C, PDT-DL can be carried out in Brazil almost throughout the year, contrary to what occurs in the European continent.
In pharmacoeconomics terms, although the commercial version of the MAL cream is 2g and the fact that major studies suggest the use of at least 1g to treat a full face,14 the authors of the present paper observed that some simple measures increase the productivity of the MAL cream (e.g. applying the product with the fingertips or a spatula) (Figure 2). The patient's facial size and profile, as well as the number and thicknesses of the AKs also have influence on the amount of cream applied to the face.
Daylight photodynamic therapy is effective in reducing the number of AK lesions on the face, with clinical improvement, even when using amounts less than half of one MAL cream tube. Thus, one tube of the product can be used in up to 4 patients, facilitating the treatment of large areas of the face with AKs. As a result, PDT-DL arises as a first line therapeutic option for the treatment of multiple facial AKs due to the feasibility of achieving clinical improvement with absence of significant local skin reactions, without the need for a specialist artificial light source device and the possibility of effectively using a single tube of MAL cream in several patients.
1. Schwartz RA, Bridges TM, Butani AK, Ehrlich A. Actinic Keratosis: an occupational and environmental disorder. J Eur Acad Dermatol Venereol. 2008;22(5):606-15..
2. Stuart J. Epidemiology of actinic keratoses and s quamous cell carcinoma. J Am Acad Dermatol. 2000; 42(1 PT 2): S4-7.
3. Olsen EA, Abernethy ML, Kulp-Shorten C, Callen JP, Glazer SD, Huntley A, et al. A double-blind, vehicle-controlled study evaluating masoprocol cream in the treatment of actinic keratoses on the head and neck. J Am Acad Dermatol 1991;24(5 pt 1):738-43.
4. Torezan L. Terapia fotodinâmica: princípios de fotoquímica, fotobiologia, agentes fotossensibilizantes e aplicações na oncologia cutânea. In: Osorio N, Torezan L. Laser em dermatologia. 2ª ed. São Paulo: Roca; 2009. p.171-94.
5. Torezan LA. Estudo da pele do campo cancerizável antes e após a terapia fotodinâmica através dos métodos clínicos, histopatológicos e imunohistoquímicos – Tese (doutorado)-Faculdade de Medicina da Universidade de São Paulo. Programa de Dermatologia. Orientador: Cyro Festa Neto. São Paulo, 2011.
6. Quaedvlieg PJ, Tirsi E, Thissen MR, Krekels GA. Actinic keratosis: how to differen- tiate the good from the bad ones? Eur J Dermatol. 2006;16(4):335-9.
7. Torezan LA, Niwa AB, Neto CF. Photodynamic therapy in dermatology: basic principles. An Bras Dermatol. 2009;84(5):445-59.
8. Grinblat BM, Festa Neto C, Sanches JA Jr, Szeimies RM, Oliveira AP, Torezan LA. Daylight photodynamic therapy for actinic kera- toses in Sao Paulo, Brazil. Photoderm Photoimmunol Photomed. 2015;31(1):54-6.
9. Wiegell SR, Haederdsal M, Philipsen PA, Eriksen P, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less pain- ful than conventional photodynamic therapy for actinic keratoses; a ran- domized, controlled, single-blinded study. Br J Dermatol. 2008;158(4):740-6.
10. Rubel DM, Spelman L, Murrell DF, See JA, Hewitt D, Foley P, et al. Daylight photodynamic therapy with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional photodynamic therapy in actinic keratosis treatment: A randomized controlled trial. Br J Dermatol. 2014;171(5):1164-71.
11. Wiegell SR, Wulf HC, Szeimies RM, Basset-Seguin N, Bissonnette R, Gerritsen MJ, et al. Daylight photodynamic therapy for acti- nic keratosis: An international consensus: International Society for Photodynamic Therapy in Dermatology. J Eur Acad Dermatol Venereol. 2012;26(6):673-9.
12. Morton CA, Wulf HC, Szeimies RM, Gilaberte Y, Basset-Seguin N, Sotiriou E, et al. Practical approach to the use of daylight photodynamic therapy with topical methyl aminolevulinate for actinic keratosis: A European consensus. J Eur Acad Dermatol Venereol. 2015;29(9):1718-23.
13. Lacour JP, Ulrich C, Gilaberte Y, Von Felbert V, Basset-Seguin N,Dreno B, et al. Daylight photodynamic therapy with methyl- aminolevulinate cream is effective and nearly painless in treating actinic keratoses: A randomized, investigator-blinded, controlled, phase 3 study throughout Europe. J Eur Acad Der- matol Venereol. 2015;29(12):2342-8.
14. Y. Gilaberte, M. Aguilar, M. Almagro, O. Correia, C. Guillén, A. Harto, B. Pérez-García, L. Pérez-Pérez, P. Redondo, I. Sánchez-Carpintero,C. Serra-Guillény L.M. Valladares.Documento de consenso hispano-portugués para el uso de la terapia fotodinámica con metil aminolevulinato y luz de día en el tratamiento de las queratosis actínicas. Actas Dermosifiliográficas. 2015;106(8):623-31.
The present study was performed at Centro de Dermatologia Dona Libânia - Fortaleza (CE), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}