


Emerson Vasconcelos de Andrade Lima
Introduction: Atrophic stretch marks constitute skin disorders characterized by the loss of collagen and elastin in the dermis, and resemble scars. Fractional lasers, microneedling and chemical peels have led to good outcomes in some cases, however there is no ideal treatment.
Objective: The objective of the present retrospective clinical study was to evaluate the effectiveness of Pulsed Radiofrequency with Multineedles (RFPM®) in late atrophic stretch marks.
Methods: A retrospective study of the safety and effectiveness of the technique was carried out by evaluating outcomes with the application of a patient satisfaction questionnaire and the assessment of clinical results by independent dermatologist physicians.
Results: A total of 8 patients (aged between 22 and 38 years) who underwent the technique were evaluated, of whom 100% reported satisfaction with the outcomes. Additionally, in the comparative evaluation of photographs carried out by two independent dermatologist physicians, the improvement rate was 50% in 2 patients and 75% in 8 patients . Post-inflammatory hyperpigmentation was observed in 10 to 20 days after the treatment in 6 patients, having been reversed after clinical treatment.
Conclusions: The new procedure is an option in the treatment of atrophic stretch marks.
Keywords: STRIAE DISTENSAE; PULSED RADIOFREQUENCY TREATMENT; COLLAGEN
The treatment of stretch marks is always a challenge, and good outcomes become even more difficult when treating old and atrophic lesions. Often resulting from skin stretching and rupture of collagen and elastic fibers in the dermis, late stretch marks arise as scars, with substantial compromise of the texture, relief and color of the involved skin.1,2
Some regions are more easily prone to stretch marks: lumbosacral and flanks in men, and abdomen, hips and breasts in women. Conditions such as pregnancy, weight gain, muscle hypertrophy and pubertal growth spurt, as well disorderly oral and topical corticosteroids, and diseases such as Cushing syndrome, are favoring factors.3
Several treatments have been proposed, offering better results in striae rubra (recent stretch marks) as compared to those obtained in striae alba (late/atrophic stretch marks). Topical tretinoin, peels, microneedling, microdermabrasion, fractional lasers and intense pulsed light are some of the treatment options used in dermatology for approaching these lesions. Nevertheless, there is no treatment that can be considered ideal, and the often poor outcomes indicate the presence of a challenge.4,5
Based on the findings obtained with the treatment of eyelids sagging, the author set out on the search for the applicability of pulsed radiofrequency with multineedles (RFPM®) in cases of old stretch marks. The present study is the result of these observations.6,7
Pulsed radiofrequency with multineedles (RFPM®)
The use of random high frequency fractional energy shot on the skin results in dermal regeneration in the papillary-reticular interface via the stimulation of fibroblasts with subsequent synthesis of collagen and elastic fibers, as well as epidermal regeneration caused by the migration of keratinocytes.
The author of the present paper proposes an innovative approach to skin rejuvenation, based on sub ablative energy delivered by electrodes with multiple needles, connected to a radioelectrosurgery device.
This technique, performed accurately and in a punctate way, it does not compromise the tissue adjacent to the vaporized microdots and causes significant tissular impact, thus enabling the stimulus for new collagen.
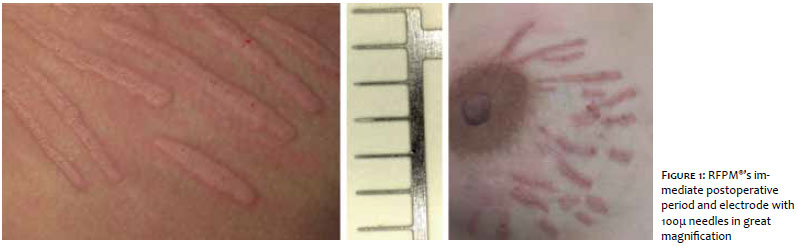
In order to perform the RFPM®, electrodes called Lima 2, Lima 4 and Lima 8 (nomenclature which refers to the author), are necessary. They respectively consist of two, four or eight tungsten needles, with a diameter of 100 thousandths of a millimeter and identical weights and lengths, arranged in parallel, in a way that they reach the same depth when in use. With 2.5mm in length, these needles will slide across the epidermis and act in the dermis, stimulating the collagen's contraction and renewal.
The objective of the present retrospective clinical study was to evaluate the effectiveness of RFPM® in late atrophic stretch marks.
Medical records of 8 female patients with atrophic stretch marks who underwent RFPM® were assessed. The procedures were performed by the same physician on an ambulatorial setting, between February and December 2015. The photographic record was carried out with the same digital camera, under the same technical conditions, immediately before and two months after a single intervention. The study was conducted according to the ethical standards of the Helsinki Declaration.
After antisepsis with 1% chlorhexidine, injections were performed in the area of the stretch marks with 2% lidocaine, without vasoconstrictor. The RFPM® application was carried out with the FRAXX® device (Loktal Medical Electronics, São Paulo, Brazil - Anvisa No. 10362610008), operating in the single pulse mode and with parameters set based on the research performed during 12 months. The patients in this group were treated with the device set on CUT mode (power = 30, active = 30ms) and the Lima 8 electrode was used, aligned with the linear path of the stretch marks. Only one pass was carried out and, in order to avoid overlapping, four parallel rows of micropunctures on average were performed with the electrode. The stretch marks must be fully treated in their thickness (Figure 1).
After the procedure the patients received dressings with micropored tape, which was removed on the following day. For the post-operative period, instructions were given for the patients to use skin regenerator (Ciclapast baume®, La Roche-Posay, Rio de Janeiro, Brazil) twice a day, in addition to commercial sunscreen SPF 60, which should be used even in covered areas.
The analysis of the outcomes was performed based on patient satisfaction questionnaires while the rating of the clinical outcomes was carried out by independent dermatologist physicians, two months after the intervention.
The patients' self-assessment questionnaire included questions about the degree of satisfaction with the procedure, measured using the categories bad, reasonable, good and very good.
The pictures of before and 60 days after the intervention were assessed by two independent dermatologist physicians, who used the following scale: regular (25% improvement), good (50% improvement), very good (75% improvement) and excellent (100% improvement).
Eight female patients between 22 and 38 years of age recruited at the author 's private practice and at the Cosmiatry Ambulatory of the Santa Casa de Misericórdia do Recife (Recife, PE, Brazil) were evaluated. The patients' Fitzpatrick phototypes ranged from II to IV. Fifty percent of the studied lesions were located in the abdomen, 30% in the buttocks and 20% in the breasts.
All patients reported satisfaction with the outcomes, attributing the good and very good ratings as answers to the proposed questions.
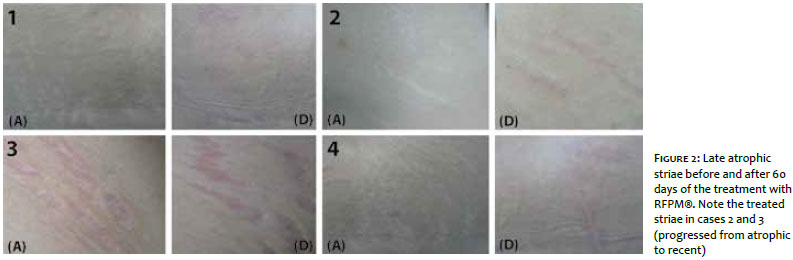
In the comparative evaluation of photographs of the before and after the procedure timepoints – which were performed by two independent dermatologist physicians – the improvement index was: 50% = good in 2 patients and 75% = very good in 6 patients (Figure 2).
The pain felt during the treatment was tolerable, and tissue regeneration could be observed between 5 and 7 days after the procedure. Return to work was possible 24 hours after. There were no occurrences of infections, dyschromias or unsightly scars in this group.
Mild to moderate post-inflammatory hyperpigmentation was observed after a period of 10 to 20 days of the treatment in 6 (of 8) patients, having been resolved in 30 to 45 days with the use of whitening formulations.
The currently large and available therapeutic armamentarium for the treatment of stretch marks provides satisfactory results in recent striae rubra, however when these lesions progress from the inflammatory phase into a late phase, with histology similar to that seen in scars with substantial degradation of collagen and elastic fibers, the treatment becomes problematic.4,5
In this way, the author of the present paper proposes the RFPM® for the treatment of late atrophic striae, a methodology thoroughly developed and studied during the last year. The technique employs specific electrodes and is based on results obtained in the treatment of periorbital aging.6 The data presented in the present article allow the authors to suggest that:
1. RFPM® is a promising therapeutic approach for the treatment of challenging lesions, such as the stretch marks
2. The obtained outcomes are reproducible using the methodology and the electrodes described in the present article
3. The prompt return to normal activities and the few adverse effects observed in the assessed group encouraged the author to recommend the inclusion of this new proposal in the broad and currently available therapeutic armamentarium for the treatment of stretch marks
4. Although reversible, post-inflammatory hyperpigmentation deserves special attention, and the author always recommends the preparation of the skin whiteners before the intervention and soon after the onset of re-epithelialization
5. The procedure requires training and is technic-dependent. The professional applying the technique must be properly qualified and posses all basic knowledge needed to ensure the excellence of the outcomes
The author suggests that the technique be assessed in other groups aiming at confirming the results and conclusions presented in this paper.
1. Osman H, Rubeiz N, Tamim H, Nassar AH. Risk Factors for development of striae gravidarum. Am J Obstet Gynecol. 2007;196(1):62-e1-5
2. 2. Elsaie M, Baumann L, Elsaaiee L. Striae Distensae (Stretch Marks) and Different Modalities of Therapy : an Update Dermatol Surg. 2009;35(4):563-73.
3. Lee SE, Kim JH, Lee SJ, Lee JE, Kang JM, Kim YK, et al. Treatment of Striae Distensae Using Ablative 10,600-nm Carbon Dioxide Fracional Laser : A Retrospective Review of 27 participants. Dermatol Surg 2010, 36(11):1683-90.
4. Bagatin E, Hassun K, Talarico S. Revisão sistemática sobre peelings. Surg Cosmet Dermatol. 2009;1(1):37-46.
5. Al-Himdani S1, Ud-Din S, Gilmore S, Bayat A. Striae distensae: a comprehensive review and evidence-based evaluation of Prophylaxis and treatment. Br J Dermatol. 2014;170(3):527-47.
6. Lima E . Radiofrequência pulsada com multiagulhas: uma proposta terapêutica em rugas, flacidez e pigmentação periorbital. Surg Cosmet Dermatol 2015;7(3):223-6.
7. Ryu HW, Kim SA, Jung HR, Ryoo YW, Lee KS, Cho JW. Clinical Improvement of Striae Distensae in Korean Patients Using a Combinated Micronnedle Radiofreuqncy and Fracional Carbon Dioxide Laser. Dermatol Surg . 2013 ;39(10):1452-58.
The present study was carried out at the Faculdade de Ciências Farmacêuticas de Ribeirão Preto, Universidade de São Paulo (FCFRP-USP) – Ribeirão Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}