


Guilherme Bueno de Oliveira1; Natália Cristina Pires Rossi2; Bárbara Maria Tarraf Moreira3
Introduction: The use of botulinum toxin in the periorbital muscles is aimed at reducing expression lines in that site, correcting the eyebrows' height and treating blepharospasm. However, the application of botulinum toxin in this area can lead to undesirable side effects, such as ptosis, edema in the lower eyelids, artificial appearance of the demarcation area between the orbicularis muscle's treated area and the malar region, ectropion and hematomas.
Objective: To treat the dynamic wrinkles in the lower portion of the orbicularis oculi muscle through injections of microdoses of botulinum toxin.
Methods: A prospective monocentric study with the analytical longitudinal observation of 300 patients undergoing treatment with botulinum toxin microdoses in the lower eyelids' rhytids was carried out. Sociodemographic data, patient satisfaction, dose quantification and complications were analyzed.
Results: Sixty-six percent of the patients showed a total improvement of the wrinkles after the first session. The other required an additional session. Eighty-six percent preferred the treatment with this therapeutic modality.
Conclusions: Despite the great benefit offered by the classic injection points for the treatment of periorbital rhytids types I to III, the authors observed the need to treat rhytids type B (presence of wrinkles on the lower eyelid). Due to the high rate of complications in this region, microdoses of botulinum toxin were proven to be effective and safe.
Keywords: BOTULINUM TOXINS, TYPE A; ESTHETICS; DERMATOLOGY
Botulinum toxin (BT) is a neurotoxin produced by Clostridium botulinum bacteria, usually found in plants, soil, and water, and in the intestinal tract of animals.1 This toxin is used to treat expression lines, and spasticity, strabismus, nystagmus and blepharospasm disorders.1,2
Botulinum toxin interferes with neural transmission, blocking the release of extracellular acetylcholine, which is the main neuromuscular junction's neurotransmitter, stimulating muscle contraction.1,3,4
Botulinum toxin Type A is the most powerful and the first BT type to be made available and used in the United States for clinical purposes. It is deemed the most powerful biological toxin to human beings.2,5
The application of BT in the periorbital muscles is used to reduce fine lines in that region, correct the height of the eyebrows and treat blepharospasm.4 This application area can develop undesirable side effects, such as ptosis, edema of the lower eyelids, artificial demarcation line between the treated area of the orbicularis muscle and the malar region, xerophthalmia, ectropion, strabismus and hematoma.4
The present study was aimed at demonstrating the treatment of the lower portion of the orbicularis oculi muscle with microdoses of BT.
A prospective, monocentric, longitudinal analytical observational study was carried out with 300 patients who underwent treatment with microdoses of botulinum toxin (Onabotulinumtoxina A - BoNT/A, Botox®, Allergan Inc., USA) in the periorbital rhytids located in lower third of the orbicular muscle of the eyes (i.e. below the zygomatic arch) at a private practice. The patients treated during this period underwent standardized digital photographs and were followed up using the private practice's proprietary medical records system.
A) Patient selection - Inclusion criteria
The patients selected for the study should mandatorily have periorbital dynamic wrinkles as their main complaint. Cases where there was presence of rhytids located in the lower third of the orbicularis oculi muscle were included.
All patients in the study should already have undergone the treatment of the periorbital dynamic rhytids with conventional application of BT, for more than six months. This criterion was important to allow the comparison of the degree of patient satisfaction between the two treatment methods (conventional x microdoses). Patients who had never undergone previous treatment in the area with BT were not included in the study.
B) Exclusion criteria
Patients with contraindication for the use of BT – such as the presence of neuromuscular diseases, including myasthenia gravis, active autoimmune conditions, pregnancy, breastfeeding, allergic reaction to the product and local infection were excluded from the study.
In addition, patients who had never undergone treatment with BT, or had been treated with BT less than six months before or who had already undergone treatment in the studied region with BT microdoses, were not selected. This exclusion criterion was important in allowing the comparison of the degree of patient satisfaction between the two methods.
c) Dilution technique
Dilution of BT for microdosing starts with the dilution of one 100 IU botulinum toxin vial (Botox®) into 2ml 0.9% saline. Two IU (0,04ml) are removed from this solution, and 10 IU (0,40ml) 0.9% saline are added, in BD Ultra Fine II® short 1ml syringe and 8mm needle, reaching a total volume of 0,48ml (12 IU). This is the final dilution, with each 0,04ml being considered one unit, which can be termed a BT microdose unit (BTMDUn).
Studied body site
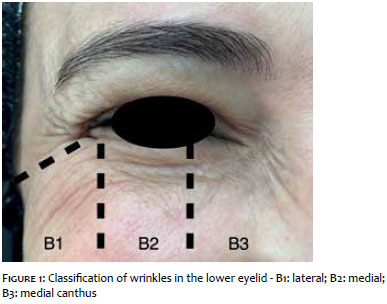
The lower third of the orbicularis oculi muscle region was defined as the region below an imaginary line originating in the lateral canthus (Figure 1). The region above this line and the remaining of the upper third of the face were treated with classic injection points.
The following classification of periorbital wrinkles,6 was used for the study:
TYPE I - wrinkles located laterally to the outer corner of the eye (lateral canthus), extending from the eyebrow up until the zygomatic arch.
TYPE II - wrinkles located laterally to the outer corner of the eye (lateral canthus), extending from the outer corner of the eye's line up until the zygomatic arch (absence of wrinkles in the upper lateral region).
TYPE III - wrinkles present only on the lateral canthus' line.
These three types of wrinkles can arise with:
A - absence of wrinkles on the lower eyelid;
B – presence of wrinkles on the lower eyelid, according to the following sub-classification (Figure 1):
B1 - lateral wrinkles,
B2 - medial wrinkles,
B3 - wrinkles in the medial canthus.
All patients selected for the study had been classified as "B" according to the above classification, with the wrinkles being sub-classified for the calculation of the number of BTMDUns needed for treating the region.
Application method and chosen dose
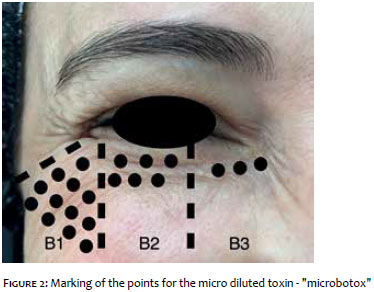
The number of micro doses used in each patient was computed according to the region's muscular strength and the formation of dynamic rhytids. After the patients were classified into types (B1, B2, B3 and B1+B2+B3 – the last classification meaning patients who had rhytids in all locations), the extent of the area with dynamic rhytids (i.e. the area to be treated, which corresponded to the whole of the region that formed rhytids resulting from movement) was determined. There were no anatomical restrictions for this study, therefore the initial points were the rhytids located closest to the orbital margin, with the inferior points respecting the last inferior rhytid. The points were marked every 0.5cm in parallel horizontal lines, marked in the craniocaudal direction.
The initial marking was of 6 to 24 points in the case of type B1 patients, 6 to 12 in the case of type B2, and 3 to 6 in type B3 (Figure 2). On the second visit (15 days after the initial application) if it was still possible to identify wrinkles in the region, additional BT micro doses were applied, according to the same pattern of distribution of points, as described above. One BTMDUn was applied in each point with a 1ml BD Ultra Fine II® short syringe and a 8mm needle. The application was carried out via intradermal route.
D) Statistical analysis
The included sociodemographic variables were gender, age, ethnicity, periorbital rhytids classification, BT micro doses used in the initial and second applications, duration, patient satisfaction compared to the previous treatment (B: better, S: similar, W: worse) and complications. The study complied with the ethical standards set out by the Helsinki declaration.
Three hundred patients were selected for the study (average age = 45, min =18, max = 72). Eighty-five percent of the study patients were female. Regarding ethnicity, 96% were Caucasian, 0.5% African-Brazilian, and 3.5% Asian. The distribution of the periorbital rhytids in the lower third of the orbicularis oculi muscle was as follows: 82% = B1, 10% = B1 + B2 + B3), 5% = B2 and 3% = B3.
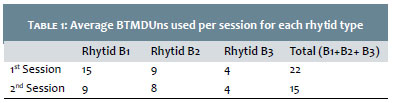
The average number of BT MD used per session for each rhytid type (for the first and second sessions) is depicted in Table 1. Thirty-four percent of the patients required a second session. The average duration of the treatment was 125 days.
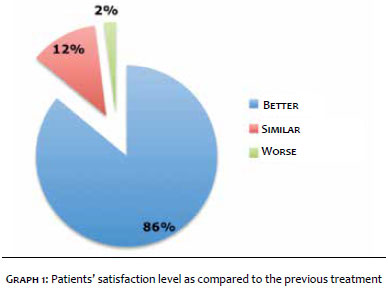
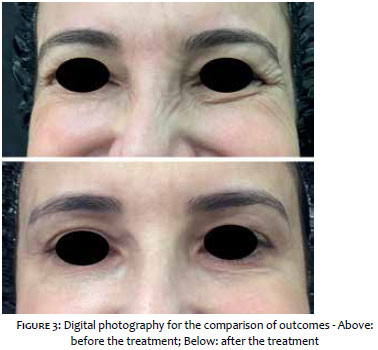
The level of patient satisfaction can be observed in Graph 1. The final outcome was recorded in digital photographs (Figure 3). Among the complications linked to the application of BT in the studied region, local pain and ecchymosis (14% and 4% of cases, respectively) were described.
The study included 300 selected patients (youngest = 18 years old, oldest = 72 years old, average patient age = 45 years). Eighty-five percent of patients were female, 96% Caucasian, 0.5% African-Brazilian, and 3.5% Asian.
The predominance of female patients in the present study is explained by the women's greater interest for cosmetic procedures, as compared to men. There are other studies in the literature demonstrating this predominance of female patients regarding similar procedures.7,8 In Brazil, the Caucasian population has greater purchasing power on average, which can be correlated with the greater demand of these patients for the treatment of rhytids in the periorbital region.7,8
The classic points for BT injection are located in the orbicularis muscle's lateral portion, having been described by Carruthers in 1998, however these points become occasionally insufficient, triggering a search for better outcomes.9 There are several published classifications for dynamic wrinkles in different facial regions, suggesting he presence of a constant search for improvement of results resulting from BT applications.10-12
The present study showed a high rate of efficacy based on the degree of patient satisfaction, with 86% of cases reporting better outcomes derived from the application of BT microdoses as compared to those achieved in previous treatments using only classic points. The analysis of complications indicated that 14% of cases had local pain while 4% had ecchymosis, converging with literature data.11 The authors highlight that in none of the 300 cases there was demarcation of an aesthetically unacceptable line between the lower eyelid and the malar region.
In line with the values found in the literature, the average treatment duration was 125 days. In his work, Costa presented an average duration of 84.5 ± 38.8 days for patients who received Toxin 1 (Botox®) and 89.9 ± 41.1 days for patients who received Toxin 2 (Prosigne®, Cristália, SP, Brazil), with absence of statistically significant difference. For the researchers, those values were 76.8 ± 46.6 and 88.1 ± 43.6 days, for Toxin 1 and Toxin 2, respectively, also with no statistically significant difference between the groups.13
The lower third of the orbicularis oculi muscle is a delicate area for treatment with BT as there is potential for many undesirable side effects, such as palpebral edema, ectropion, xerophthalmia and, in special, the formation of a demarcation line with artificial aspect between the treated area of the orbicularis muscle and the malar region, with unsightly aesthetic outcome. Even with the great benefit lent by the classic points in the treatment of types I to III periorbital rhytids, the authors verified the need for the treatment of type B rhytids. Due to the high rate of complications intrinsic to the studied region, BT microdoses were effective and safe for the treatment of that body site.
1. Nigam PK, Nigam A. Botulinum Toxin. Indian J Dermatol. 2010;55(1): 8-14.
2. Baumann L, Elsai M L, GRUNEBAUM L. Botulinum Toxin. In: Baumann L. Cosmetic Dermatology: principles and practice. Mcgraw-Hill Profession- al: New York, 2009. p.169-80.
3. Dressler D, Saberi FA, Barbosa ER. Botulinum toxin: mechanisms of action. Arq Neuropsiquiatr. 2005; 63(1):180-5.
4. El-Minawi H, Elshazly MI, Zayed AA. The effect of Periorbital Botox Injection on the Eye. Kasr El Aini J Surg (Cairo). 2010;11 (3): 61-6.
5. Hsu YC, Wang HJ, Chuang YC. Intraprostatic Botulinum Neurotoxin Type A Injection for Benign Prostatic Hyperplasia. Open Access Toxinol J. 2016;8(5):126.
6. Tamura BM, Odo M Y. Classification of periorbital wrinkles and treatment with Botulinum Toxin Type A. Surg Cosmet Dermato. 2011;3(2): 129-34.
7. Webster RC, Hamdan US, Gaunt JM, Fuleihan NS, Smith RC. Rhinoplastic revi-sions with injectable silicone. Arch Otolar- yngol Head Neck Surg.1986;112(3):269-76.
8. Villarejo Kede MP, Sabatovich O. Ácido Hialurônico: Preenchimento de contor-no nasal. 3ª ed. Rio de Janeiro: Atheneus, 2015.
9. Carruthers A, Carruthers J. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1189-94.
10. Almeida ART,Marques ER, Kadunc BV.Glabelar wrinkles:a pilot study of con-traction patterns. Surg Cosmet Dermatol. 2010;2(1):23-8.
11. Tamura BM, Odo MY, Chang B, Cucé LC, Flynn TC. Treatment of nasal wrin-kles with botulinum toxin.Dermatol Surg. 2005:31(3)271-5.
12. Braz AV,Sakuma TH.Patterns of contraction of the frontalis muscle. Surg Cosmet Dermatol. 2010:2(3):191-4.
13. Costa A, Talarico Filho S, Arruda LH, Pecora CS, Ortolan DG, Monteiro EO, et al. Multicenter, prospective, comparative, randomized, double-blind clinical study comparing two botulinum toxin type A formulations registered in Brazil for the treatment of glabellar wrinkles. Surg Cosmet Dermatol 2016;8(1):33-40.
The present study was performed at the authors' private practices in São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}