


Fabiane Mulinari-Brenner1; Donelle Cummings2; Betina Werner3; Marina Riedi Guilherme4
Hyaluronic acid is the currently most used filler in dermatology due to its low risk of adverse events. The objective of this study is to report a case of granulomatous reaction after filling with two types of hyaluronic acid, in the perioral region and in the nasolabial folds. A female patient with rheumatoid arthritis treated with leflunomide presented onset of symptoms 30 months after filling. Autoimmune diseases may facilitate the occurrence of complications and should be followed carefully before filling with hyaluronic acid. As already reported with the use of interferon and omalizumab, granulomatous reaction to fillers may occur after use of leflunomide.
Keywords: HYALURONIC ACID; GRANULOMA; RHEUMATOID ARTHRITIS; FOREIGN-BODY REACTION
Ideal cutaneous filling substances have low incidence of complications, low potential for allergenicity and inflammatory reactions, lasting effects, absence of migration, are easy to apply and cost effective. Products with profiles that more closely resemble that one are derived from hyaluronic acid (HA). Despite being generally safe, cases of granulomas and other complications have been described following filling procedures with HA. The present paper describes a case of a granulomatous reaction following a filling procedure, associated with the beginning of use of leflunomide.
The patient "MRS", a 59 year-old woman, had complaints of perioral wrinkles. She had a history of well-controlled rheumatoid arthritis and Sjögren syndrome. In May 2007, after having signed a Free and Informed Term of Consent, she underwent a deep dermal filling with a high viscoelastic HA based gel in the nasogenian fold and a superficial dermal filling with a lower viscosity gel in the superior perioral region. The patient was satisfied with the outcome, however a slight overcorrection in a transverse groove to the left of the upper lip was noticed2 weeks after the procedure. A palpable papule of 0.3cm in diameter proved persistent in the 3-month reevaluation after the procedure. As it was barely noticeable, a decision was made for observing its development. Nevertheless, the papule persisted in the 19-month review consultation of the lesion in the left supralabial region.
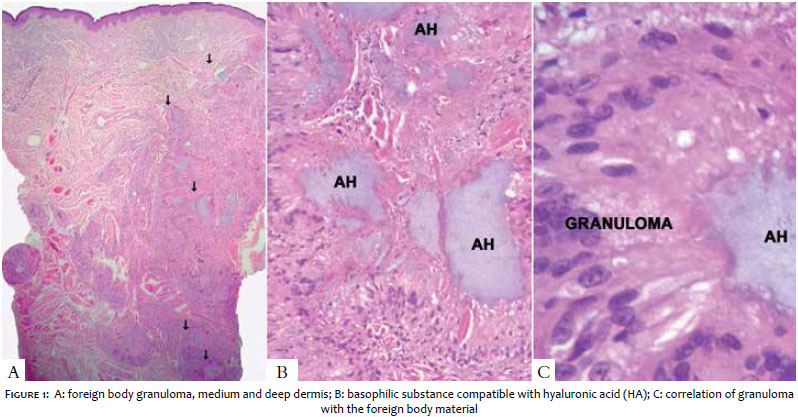
Thirty months after the procedure, the patient returned due to the emergence of multiple nodules in the supralabial region bilaterally, with a 2-week development and progressive increase. She denied having undergone other aesthetic procedures in the region since the initial filling. The patient also reported worsening of the rheumatoid arthritis picture 4 months before, with an increase of prednisone to 20mg/day for 2 weeks and the beginning of 20mg/day leflunomide. A biopsy of the nodular lesion suggested the presence of a chronic foreign-body granulomatous dermatitis affecting the superficial and deep dermis. An amorphous material compatible with HA was observed in the center of the reaction (Figure 1). A treatment was proposed with intralesional injection of hyaluronidase, however the patient rejected it. A systemic corticosteroid therapy was then prescribed, with oral prednisone 1 mg/kg for 2 weeks and 0.5 mg/kg for 2 additional weeks, associated with the suspension of leflunomide, with improvement of the picture.
Hyaluronic acid is considered the safest dermal filler, with good cosmetic response. It is a natural polysaccharide – an important structural element of the skin, subcutaneous, connective tissue and synovial fluid. It belongs to a group of a few substances that are identical in all living beings. It acts by adding volume to the tissues and restoring contours.Yet, there are some cases of side effects caused by the product. 1
Interferon and new immunomodulators can produce granulomatous reaction in patients with dermal fillers, both with HA and calcium hydroxyapatite. Although this complication is rarely reported and the filler used is often difficult to identify, this seems to be the first case described with leflunomide, with the fact that the patient had been followed up since the initial procedure simplifying the diagnosis.
Leflunomide interferes with the hyaluronic acid synthase, suppressing the production of HA in the fibroblast-like synoviocytes in a dose-dependent effect, aiding in the treatment of rheumatoid arthritis. Little is known about its interference in the skin's HA. The use of leflunomide – as well as of methotrexate – in patients with rheumatoid arthritis favors the development of a granulomatous response with increased frequency of rheumatoid nodules. 2
In the present case, it was not possible to exclude the hypothesis that the frequent use of systemic corticosteroids may have masked a preexisting granuloma, nevertheless the rapid progress after the start of leflunomide and the improvement after its suspension suggest the involvement of this drug in the process. A deviation of the T helper 2 immunity (Th2) to Th1 can explain the granulomatous reaction as described in granulomas induced by interferon. 3 Another possibility is that an increase in the corticosteroid dose followed by rapid reduction may contribute to this process, despite the fact that the patient has denied taking prednisone doses greater than 20 mg/day.
Regarding the association with rheumatoid arthritis, some reports suggest the relative contraindication of filling procedures with HA in patients with lupus erythematosus and collagen diseases, nonetheless there is absence of descriptions mentioning rheumatoid arthritis.
By comparing the physical properties of HA-based cutaneous fillers, such as fluid gel proportion, HA modification extent, cross-linking percentage, particle size and module, it is possible to define the product's behavior and the depth to which it should be applied for a better clinical response. 4 For this reason, two different types of HA were used in the patient, with both apparently leading to reactions, since all filled areas were affected.
Comparing various cutaneous fillers, HA is an excellent choice for increasing lip volume and perilabial volumes due to its hydrophilic properties in the tissues.3 The fillers containing non-animal origin HA can cause hematoma, edema and erythema more often. These complications are most common in the labial region, due to increased vascularization and tendency to edema in this area. Both of the fillers used in the present study were not derived from animals. The Restylane® line of products (QMed AB, Uppsala, Sweden) are produced by fermentation of Streptococcus cultures, partially cross-linked by Nasha technology (Non animal-stabilized hyaluronic acid). The product Restylane Fine Lines® has 20mg/ml HA and is indicated for the treatment of fine superficial wrinkles, such as the one in the perioral region. The Perfectha Deep® is HA based gel with high viscoelasticity, used in deeper wrinkles, such as the ones in the nasogenian folds. It contains 24 mg/ml HA, stabilized by hydrogen bonds, which allow the formation of a stable gel. The products were used at appropriate levels of injection. Both have low amounts of protein and endotoxin (<0.25 IU/g), with rare hypersensitivity reactions.
Side effects caused by cutaneous fillers are divided into intermediate (from 1 to 12 months after the procedure) and long term (12 months after the procedure). 3 Intermediate side effects involve local effects (edema, angioedema, skin induration, nodules) or systemic effects (fever, arthralgia, arthritis, skin and eye lesions, and dry mouth). Pain, erythema, edema and ecchymosis are expected during the first 2 weeks, however persistent edema has been reported. 5 In cases of granuloma caused by HA in the first weeks after filling, it is hypothesized that there is induction due to contamination by a protein during the procedure, possibly by the biofilm created around the implantation site. 6 Among the long-term side effects, granulomatous reactions are the most feared. Trauma and injection of other filling substances in the same location of the HA are possible causes for the onset of the process. In the present case, however, in addition to the late onset, the patient has denied undergoing any other procedure or aggression in the site over the past 30 months, ruling out these triggering factors. Late granulomatous or inflammatory reactions without associated factors have been reported in some cases after multiple HA injections.3, 7 In most cases described, reactions have arisen within 18 months of the filling procedure, though they can occur up until 36 months, during the enzymatic degradation period.7 In the present case, 30 months were required for the onset.
Despite the fact that late reactions to HA had persistent or recurring form in more than 20% of cases, an improvement of symptoms was observed in the present case as a result from systemic corticosteroid therapy, without recurrence. 3
The ideal filler is still utopian, and it is necessary to evaluate risks and benefits on a case-by-case basis. It is indispensable that the patient be informed on the potential risks in advance. Rheumatoid arthritis, as well as the use of drugs such as leflunomide, might facilitate the occurrence of complications and should be contraindications for HA based filling procedures. Although uncommon, complications caused by HA implants can occur late on, after the average duration of the degradation period (18 months after the filling procedure).
1. Park HJ, Jung KH, Kim SY, Lee J-H, Jeong JY, Kim JH. Hyaluronic acid pulmonary embolism: a critical consequence of an illegal cosmetic vaginal procedure. Thorax. 2010;65(4):360-1.
2. Stuhlmeier KM. Effects of leflunomide on hyaluronan synthases (HAS): NF-kappa B-independent suppression of IL-1-induced HAS1 transcription by leflunomide. J Immunol. 2005;174(11):7376-82.
3. Bitterman-Deutsch O, Kogan L, Nasser F. Delayed immune mediated adverse effects to hyaluronic acid fillers: report of five cases and review of the literature. Dermatology Reports [Internet]. 2015;7(1):12-4.
4. Kablik J, Monheit GD, Yu L, Chang G, Gershkovich J. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol Surg. 2009;35(Suppl. 1):302-12.
5. Arron ST, Neuhaus IM. Persistent delayed-type hypersensitivity reaction to injectable non-animal-stabilized hyaluronic acid. J Cosmet Dermatol. 2007;6(3):167-71.
6. Mamelak AJ, Katz TM, Goldberg LH, Graves JJ, Kaye VN, Friedman PM. Foreign body reaction to hyaluronic acid filler injection: In search of an etiology. Dermatol Surg. 2009;35(Suppl. 2):1701-3.
7. Sage RJ, Chaffins ML, Kouba DJ. Granulomatous foreign body reaction to hyaluronic acid: Report of a case after melolabial fold augmentation and review of management. Dermatol Surg. 2009;35(Suppl. 2):1696-700.
This study was carried out at Hospital de Clínicas da Universidade Federal do Paraná (UFPR) – Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}