


Beatriz Lopes Ferraz Elias1; Flávia Regina Ferreira2; Elisângela Manfredini Andraus de Lima3; Carolina Forte Amarante4; Samuel Henrique Mandelbaum5
Vitiligo is an acquired depigmentation characterized by partial or total loss of epidermal melanocytes. Many therapeutic modalities have been proposed for its treatment. In cases of stable vitiligo surgical treatments are preferred. Grafting by epidermal scraping is a variant of micrografts by punch technique. It is a new, simple and low cost technique, with high rates of repigmentation. The objective of this report is to demonstrate the authors' experience with this technique and discuss the results in an initial series of two cases (three lesions).
Keywords: PHOTOTHERAPY; VITILIGO; PIGMENTATION DISORDERS; DERMABRASION; MELANOCYTES
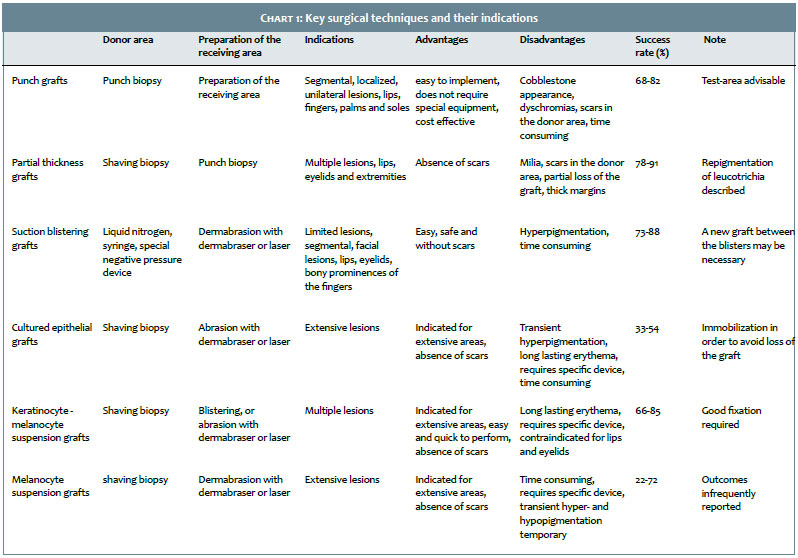
Vitiligo is a disorder consisting of acquired depigmentation that is aesthetically disfiguring and characterized by partial or total loss of epidermal melanocytes. It affects from 0.5% to 1% of the world population.1 It arises as hypo- or achromatic macules, usually bilateral and symmetrical. It can be classified into different clinical forms: vulgaris, acrofacial/acral, focal, mucosal, segmental and universal.2 Many therapeutic modalities have been proposed for its treatment. In stable cases of vitiligo – defined by the absence of both new lesions (or the progression of existing ones) and the Koebner phenomenon for at least one year, surgical treatments are preferred.3 Surgical treatments have been described since 1964, and numerous techniques have been developed.4 The choice of the method depends on the location of the lesions, the extent of the picture, skin phototype of the patient and the experience of the surgeon. Chart 1 describes the main surgical techniques and indications. The epidermal scraping grafting technique is a variant of the punch micrografting technique. It is a new, simple and cost effective technique that leads to high rates of repigmentation. Its outcome is compared to that of the transplantation techniques with culture of melanocytes.3 Despite the fact that it is a technique that has been developed more recently, it is already widespread in some countries – in India for example. The objective of the present report is to demonstrate the authors' experience with this technique and discuss the outcomes obtained with an initial series of two cases (three lesions).
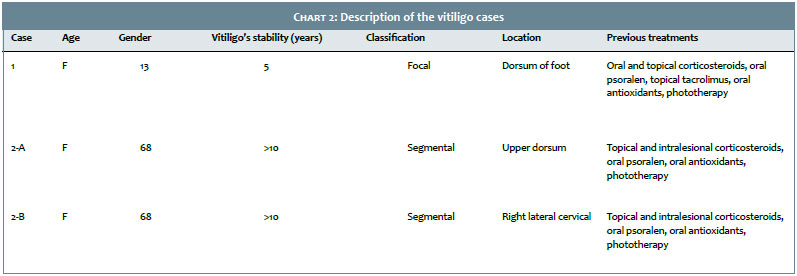
1- Description of cases: Epidemiological (gender, age, skin color) and clinical information (duration of stability, classification and location of the vitiligo), and previous treatments of the patients involved in this study are in Chart 2.
2 - Description of the technique:
Donor area (lumbosacral region).
The antisepsis was performed with aqueous chlorhexidine and local anesthesia injection was carried out with 2% lidocaine.
With the skin stretched, thin tissue slices were obtained using sterile razor blade (with firm and smooth upward and downward movements). The tissue obtained should ideally be thin enough to allow that the inscription imprinted on the blade be read through transparency. This tissue was then placed in a sterile container with saline and fragmented with a delicate scissors for about 20 minutes, up until a homogeneous consistency was obtained (Figure 1).
The dressing of the donor area should not be adherent and prepared with petrolatum gauze, with patients being instructed on the local hygiene and the daily change of the dressing.
Receiving area
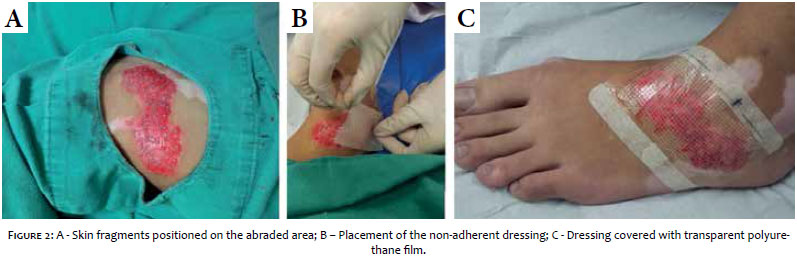
Antisepsis and local anesthesia were performed similarly to the procedure carried out in the donor area. The receiving area was then manually dermabraded with sandpaper up until it reached the point of pinpoint bleeding. The obtained exudate should not be removed. The material obtained from the donor area was subsequently placed on the abraded area, within the limits of the lesion (Figure 2A).
The area was covered with non-adherent open mesh cotton dressing soaked in paraffin and chlorhexidine, and then finalized with a transparent polyurethane film (Figures 2B and 2C).
Patients should be instructed not to wet the dressing and immobilize the treated area for seven days. After that period, careful local hygiene should be carried out daily.
3 - Development:
Fifteen days after the procedure, phototherapy of the treated area was started with narrow band ultraviolet B (NB-UVB), being performed twice a week.
The follow-up visits took place at weeks 0, 2, 8 and 18, with photographic records being carried out.
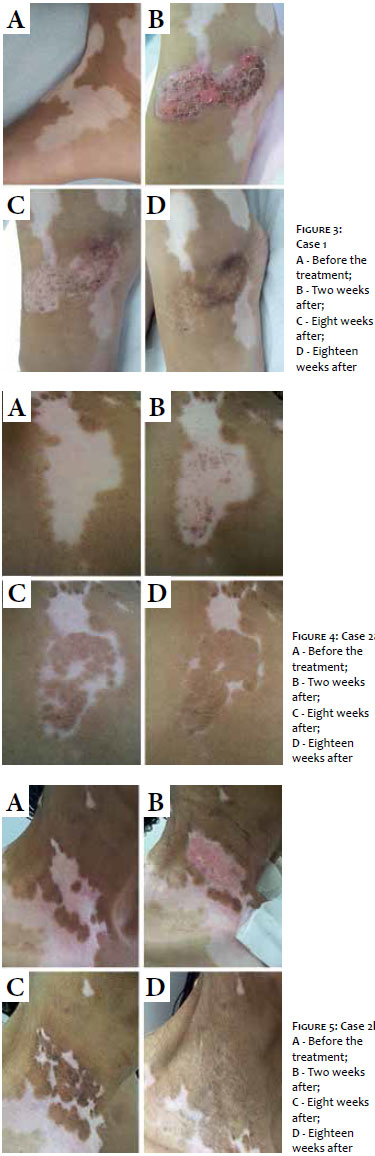
From the second week it was already possible to observe uniform epithelialization of the treated area. In both cases the authors obtained good outcomes (uniform pigmentation present in virtually the entire area treated in addition to homogeneous pigment with color similar to the adjacent area), and a high repigmentation rate (Figures 3 to 5).
It was also possible to observe the complete epithelialization of the donor area (Figure 6). Both patients are being followed up at the Dermatologic Clinic, undergoing phototherapy sessions and maintaining the results obtained.
The epidermal scraping grafting technique is very simple, easy to perform, does not require expensive materials or equipment and provides high rates of repigmentation. The main advantage of this method as compared to the original punch micrografting technique is that it does not lead to the "cobblestone" aspect in the treated area, dyschromias in the donor and recipient areas, elevation of the grafted area, poor healing of the donor area and, in special, limitation in the extensibility of the donor area.3, 5
The epidermal scraping grafting technique can be performed on extensive areas due to the homogeneous consistency of the material laid on the area to be treated. Studies show that the donor area can be up to 1/10 of the receiving area's size. 3
Regarding the donor area, the most used locations are the thighs, buttocks and lumbosacral region due to the fact that they are photoprotected areas and obtaining tissue from them is straightforward. In general, the donor area has fast and satisfactory epithelialization. Nevertheless, post-inflammatory hyperpigmentation, hypertrophic scars and unsightly scars may occur, depending on the individual healing process and the surgeon's skills.3
The receiving area can be prepared using several techniques, such as dermabrasion, laser abrasion, and blistering induction by suction or liquid nitrogen. 5 In the present study, the authors chose to use the manual dermabrasion with sandpaper technique. The acral regions and the areas over the joints should be avoided – especially in very young patients – for it is considerably difficult to implement the techniques in these locations and there is risk of treatment failure. In addition, the receiving area should be dermabraded only until the pinpoint bleeding emerges in order to avoid unsightly scars. Among the complications reported in the receiving area are: dyschromias, infections and local pain.3
There was absence of complications in the present study. Patients should be properly instructed regarding the post-operative care. The treatment area should be kept immobilized and covered with a dry dressing for one week. After this period (when the dressing should be removed), it is important to provide guidance about the expected clinical aspect and instructions on the need for meticulous daily cleansing, aiming at allowing the spontaneous peel off of the crusts. Despite the small number of references on this fact, the high rate of repigmentation obtained with this technique is a consensus in the literature.1, 3, 6, 7 Studying 26 patients, Krishnan et al.3 achieved repigmentation rates of 90% five months after the treatment.
Yet, the reason for the success in achieving high pigmentation rates with this technique is still unknown7 and some authors have questioned whether the obtained pigment is a result of the transfer of melanocytes or of post-inflammatory hyperpigmentation, without diffusion of melanin.5
Other studies show that the abraded area would be of crucial importance for the success of the procedure since it produces growth factors, such as the vascular endothelial growth factor, which is important for the epithelialization and repigmentation processes.3, 8
It is also believed that melanocytes are not absent in vitiligo; rather, they would be inactive and a stimulus, such as curettage or, as was the case in this study, abrasion, would encourage the transcription of the tyrosinase gene, through the activation of the c-kit receptor by the cytokines induced by the stimulus.9, 10
Finally, the combination of the stimulus with the transfer of melanocytes and keratinocytes appears to be more effective than the isolated stimulus. While the difference was not statistically significant, Quezada et al.6 demonstrated the presence of a faster response and a more uniform pigmentation of the treated area with dermabrasion associated with the transfer of melanocytes and keratinocytes as compared to the isolated abrasion.
Vitiligo is a condition with great psychosocial impact and surgical treatments have proved promising for their positive effect in the therapeutic response of recalcitrant cases. The epidermal scraping grafting technique has high repigmentation rates and does not require expensive technology, which has motivated the authors in the present study, corroborating the literature and helping to disseminate this technique.l
1. Sahni K, Parsad D, Kanwar AJ, Mehta SD. Autologous noncultured melanocyte transplantation for stable vitiligo: Can suspending autologous melanocytes in the patients' own serum improve repigmentation and patient satisfaction?. Dermatol Surg. 2011;37(2):176-82.
2. Nakamura RC, Azulay-Abulafia L, Azulay RD. Discromias. In: Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. Rio de Janeiro: Guanabara Koogan; 2011. p. 97-114.
3. Krishnan A, Kar S. Smashed skin grafting or smash grafting - a novel method of vitiligo surgery. Int J Dermatol. 2012;51(10):1242-7.
4. Gawande V, Kar S, Gupta D. Surgeries in vitiligo - A review article. J MGIMS. 2011;16(2):20-4.
5. Issa CMBM. Transplante de melanócitos no tratamento do vitiligo: Um progresso terapêutico?. [tese]. Campinas: Universidade Estadual de Campinas; 2003.
6. Quezada N, Machado Filho CA, De La Sotta P, Uribe P. Melanocytes and keratinocytes transfer using sandpaper technique combined with dermabrasion for stable vitiligo. Dermatol Surg. 2011;37(2):192-8.
7. Van Geel N, Ongenae K, Naeyaert JM. Surgical Techniques for Vitiligo: A Review. Dermatology. 2001;202(2):162-6.
8. Howdieshell TR, Riegner C, Gupta V, Callaway D, Grembowicz K, Sathyanarayana, et al. Normoxic wound fluid contains high levels of vascular endotelial growth factor. Ann Surg. 1998; 228(5):707-15.
9. Zanini M, Wulkan C, Machado Filho CA. Vitiligo: há ou não melanócitos? Med Cutan Iber Lat Am. 2002;30(4):152-3.
10. Machado Filho CA, Almeida FA, Proto R. Vitiligo: analysis versus curettage alone, using melanocytes morphology and reverse transcriptase polymerase reaction for tyrosinase mRNA. Sao Paulo Med J. 2005;123(4):187-91.
This study was carried out at the Dermatology Service of the Hospital Universitário de Taubaté - Taubaté (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}