


Daniel Nunes e Silva1; Byanca Rossetti Moreira dos Santos2; Luciano Ipólito Branquinho2; Marcus Machado de Melo2; Marcelo Rosseto3
Rhinophyma tends to determine important nasal changes, with aesthetic and functional impairment, especially in more advanced cases. Despite the various techniques already described, the search for the ideal treatment persists. Two patients with rhinophyma underwent tangential excision associated with electrocoagulation, with subsequent intensive cosmetic treatment. The described technique is effective, safe, with excellent aesthetic results and no recurrences during the study period. This proposed combined treatment appears as a great alternative for the treatment of rhinophyma due to its technical simplicity and its good long-term results.
Keywords: RHINOPHYMA; ELECTROCOAGULATION; NOSE DISEASES
Rhinophyma is a benign cutaneous lesion of slow growth and potentially disfiguring that affects the nose. It leads to hyperemia and telangiectasia, causing dilated pilosebaceous pores, increased volume and nodule formation in the region. These changes may lead to the complete deformation of the nose, entailing functional, aesthetic and psychological consequences to patients.1 It is histologically characterized by hyperplasia of sebaceous glands and fibrovascular proliferation of the nasal dermis.1,2 Its etiology has not yet been fully elucidated.1, 2 Some authors believe that rhinophyma is correlated to centrofacial rosacea stage IV, being considered an uncommon subtype (3.7%) by them.1,3 Others believe that the condition is an entity on its own for, unlike rosacea, it predominates in men and can manifest in the absence of the typical acneiform picture. Some risk factors for its development are described in the literature: exposure to sunlight, age (men over 40 years of age), alcoholism and stress.1 Surgery for rhinophyma resection dates back to the 19th century, when Von Langerbeck performed a complete resection of the skin, leaving it to heal by secondary intention.4 Total skin grafts were also widely used in the recent past. 5 Innovative less aggressive treatments, such as dermabrasion, cryosurgery, CO2 or argon laser ablation, and trichloroacetic acid have been recommended by most authors.1, 3, 4, 6 Despite the various techniques already described, there is still no gold standard for the surgical treatment of rhinophyma.7 The search for the best therapeutic option continues, especially for the most advanced cases, where good aesthetic outcomes are not always achieved with less aggressive treatment options.7, 8 Although it has been used for many years, tangential resection associated with electrocoagulation is a simple and safe technique that does not require the use of complementary technology. There is abundant literature regarding the variety of proposed postoperative cosmiatric treatments, however there is consensus on the fact that when carried out intensely and in a sustained manner, they can lend superior results in both functional and aesthetic aspects.4 The objective of the present study is to describe the results obtained in patients with rhinophyma treated with the combination of surgery and postoperative cosmiatric care.
Two patients bearing rhinophyma were treated with the method proposed below, at the author's private clinic in 2009. The tangential excision technique combined with electrocoagulation, with the subsequent cosmetic treatment was performed in a hospital setting, under fentanyl and midazolam-based light sedation, as described below (Figure 1). The author opted for the use of local anesthesia in the nasal area with the injection of roughly 20 ml of solution containing 0.125% lidocaine and 1:200,000 epinephrine. The tangential resection was performed with a number 24 scalpel blade, removing linear segments of varying thickness (1mm to 2mm) from across the affected region, observing the nasal aesthetic units. After the entire surface had been treated in this manner, the vigorous electrocoagulation of the bloody area with traditional electrocautery. At the end of the procedure the wound was covered with collagenase ointment, with the patient being discharged about four hours later. Instructions were given for the application of collagenase ointment 4 times a day during the first 30 days, with weekly visits to the practice for reassessments with the surgeon. A humectant re-epithelizing lotion composed of essential fatty acids; medium chain triglycerides, vitamins A and E began to be applied on the 30th day, associated with the frequent use of a diverse lotion containing a high sun protection factor. On the 60th day after the surgery, a silicone-based gel was introduced, with six applications per day, associated with the overnight coverage of the lesion with a silicone gel sheet. This conduct was maintained up until the 6th postoperative month. After this period, the patients continued to use only the lotion containing sunscreen for another 6 months (Figure 2).
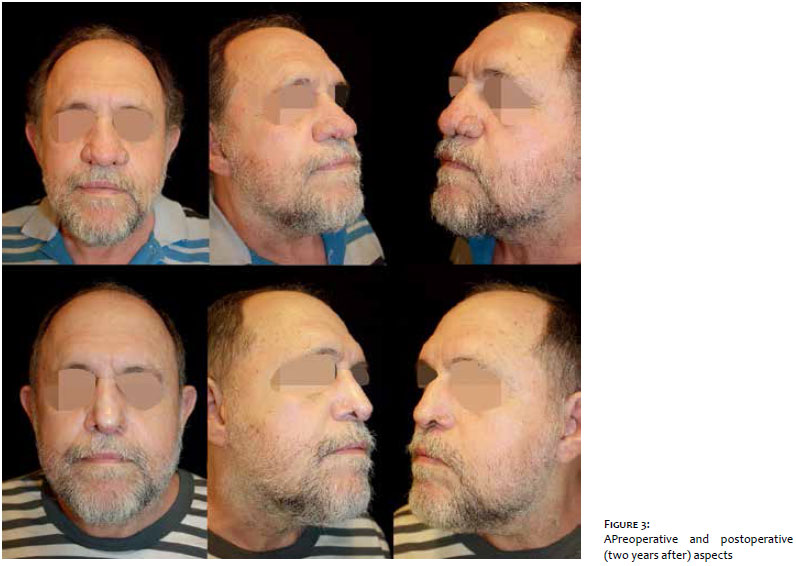
Patient 1: Mr. "JLC", 59 years old, white, diabetic, non-alcoholic, presenting thickening of the nose, nodules, telangiectasia, dilation of pilosebaceous pores for 3 years (Figure 3).
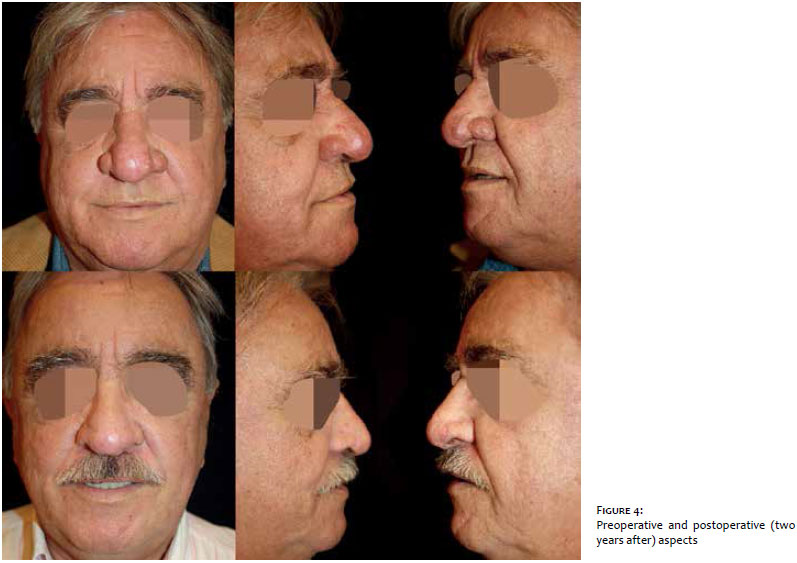
Patient 2: Mr."LT", 54 years old, white, alcoholic, presenting erythema, telangiectasia, cutaneous thickening and dilation of pilosebaceous pores in the external nasal area, with two years of development (Figure 4).
Much remains to be discussed about the treatment of rhinophyma. 2 Several interesting options – surgical or not – are available in the literature. Nevertheless, the need for more effective, less aggressive alternative techniques that lead to better results is reported by various authors for years, especially for more advanced cases of the condition.2, 9 The use of topical treatments – such as trichloroacetic acid – and ablative techniques – such as CO2 laser and RF – have emerged in recent years as non-surgical alternatives for the treatment of rhinophyma.1 The latter use ablation of the lesion associated with cauterization of the wound, promoting adequate hemostasis, technical precision and less tissue destruction.2, 9 These procedures, however, are more time consuming, rely on technology and/or proper training, which are not always available to all physicians. Moreover, the outcome can be different from that one obtained with the combined technique, especially in severe cases.4, 9, 10 The results described in the present study demonstrate that an established technique, such as tangential excision, combined with electrocoagulation, can be improved based on the association of simple, cost effective and easy to perform cosmetic treatments. The topical treatment with collagenase (used in the initial postoperative period) ensured the cleansing of the treated areas, enzymatically dissolving necrosis and crusting.In addition, it also promoted the formation of granulation tissue.11 It is commonly reported that re-epithelialization of the wound after electrocoagulation takes between 10 and 15 days.7 In the present study, the use of such technique reduced scarring and deformity, and accelerated the re-epithelialization from the remaining sebaceous glands. 8 The association with sunscreen may have prevented the undesirable hyperpigmentation described in the conventional technique.2 Several authors advocate the prolonged use of sunscreen in cases of rhinophyma, since irritating factors, such as ultraviolet radiation, can contribute to the progression of rosacea.4 Furthermore, exposure to the sunlight can trigger the hyperpigmentation of the lesion due to its intense proinflammatory effect. 12 None of the patients experienced worsening of the lesion or local irritation caused by the use of sunscreen. Among the potential complications of electrocoagulation, which were not observed in the present study, are the formation of unsightly scarring, and asymmetry and perforation of the nasal cartilage.8 Covering the lesion with the silicone gel plate promoted an increase in the local temperature and strengthened the action of endogenous collagenase, allowing the final resolution of the scar, preventing its hardening and reducing the degree of contraction.13 The combined use of the ointment and silicone plate improved the final appearance of the wound, minimizing the risk of complications described in the conventional technique.8 The final results obtained in patients treated with this method have been achieved due to the combination of the beneficial effects provided by the use of various cosmiatric techniques – some already established in the literature, others still requiring further studies. 4 Still, each of them played a key role in the successful treatment and maintenance of the outcomes, which remained stable for a period in excess of 5 years, demonstrating the safety and effectiveness of the method.
The combination treatment described in the present study arises as an excellent alternative for the treatment of rhinophyma due to its technical straightforwardness and good longterm results.
1. Reyes JAE, Valencia DPP. Rinofima: una revisión de la literatura. Acta de Otorrinolaringología & Cirugía de Cabeza y Cuello. 2012;40(3):220-7.
2. Mancera CJ, Cervantes HD, Monroy ZJ, Izquierdo OC. Rinofima: Tratamiento quirúrgico con el uso de radiofrecuencia. Cir Plast. 2007;17(3):176-80.
3. Khaled A, Hammani H, Zeglaoui F, Tounsi J, et al. Rosacea: 244 Tunisian cases. Tunis Med 2010;88:597-601.
4. Rohrich RJ, Griffin JR, Adams WP Jr. Rhinophyma: review and update. Plast Reconstr Surg. 2002;110(3):860-9.
5. Polat K, Uysal IÖ, Karakus CF, Altuntas EE, et al. The treatment of rhinophyma with excision and full-thickness skin graft. Cumhuriyet Med J. 2012;34:504-9.
6. Gaspar NK, Gaspar APA, Aide MK. Rinofima: tratamento prático e seguro com ácido triclcoroacético. Surgical & Cosmetic Dermatology. 2014;6(4):368-72.
7. Bogetti P, Boltri M, Spagnoli G, Dolcet M. Surgical treatment of rhinophyma: a comparison of techniques. Aesthetic Plast Surg. 2002;26(1):57-60.
8. Rordam OM, Guldbakke K. Rhinophyma:Big problem, simple solution. Acta Derm Venereol. 2010;11:188-9.
9. Greenbaum SS, Krull EA, Watnick K. Comparison of CO2 laser and electrosurgery in the treatment of rhinophyma. J Am Acad Dermatol. 1988;18:363-8.
10. Baker, TM. Dermabrasion. As a complement to aesthetic surgery. Clin. Plast. Surg. 1998;25:81-8
11. Jung W, Winter H. Considerations for the use of Clostridial Collagenase in Clinical Practice. Clin Drug Invest. 1998;15(3):245-52.
12. Juchem PP, Hochberg J, Winogron A, Ardenghy M. Riscos à Saúde da Radiação Ultravioleta. Rev Bras Cir Plást. 1998;13(2):31-60.
13. Borgognoni L. Biological effects of silicone gel sheeting. Wound Repair Regen. 2002;10(2):118-21.
This study was carried out at the Universidade Federal de Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}