


Aracele Silva Cardoso1; Danilo Augusto Teixeira2; Bruna Vicente de Oliveira3; Priscila Prais Carneiro3; Rafael Ferreira Junqueira4
Use of botulinum toxin type A in first intention healing wounds has been widely adopted in order to inhibit the formation of hypertrophic scars. In this report we demonstrate the use of the toxin in a surgical wound left to heal by secondary intention, after the removal of a squamous cell carcinoma in situ by Mohs micrographic surgery in supralabial region, with good cosmetic result. Botulinum toxin acts by inhibiting the proliferation of fibroblasts, by differentiating fibroblasts and by producing type I collagen, which are the main factors responsible for the good quality of the healing process.
Keywords: BOTULINUM TOXINS, TYPE A; CICATRIX; WOUND HEALING; CARCINOMA, SQUAMOUS CELL
Scars are a major concern for patients, especially if located in the face.1 They are unavoidable consequences of surgical treatments in general.1 An important factor that can hamper the sound development of the healing process is the presence of tension in the wound's borders. The facial muscles and their connections with the skin promote continuous tension on the surgical wound, impairing the final cosmetic outcome. 2
Botulinum toxin type A has been shown to be a good option for optimizing the healing process. 3 It is a powerful neurotoxin produced by the bacterium Clostridium botulinum, an anaerobic rod cell, which promotes inhibition of acetylcholine release at the neuromuscular junction. In the 1970s, Scott was the first to propose the use of the toxin as a medical therapy for the treatment of strabismus.2
After undergoing endocytosis at the nerve terminal, the toxin promotes inhibition of acetylcholine release at the neuromuscular junction, suppressing muscle contraction for a period of two to six months. 3, 4 When applied to cutaneous wounds, it reduces tension in the wound's borders, providing aesthetic gain.5
There are many reports of toxin use for primary sutures, but few records of its use in healing process by secondary intention. In the present report, the authors describe the case of intraoperative application of botulinum toxin followed by secondary intention healing, with excellent aesthetic results.
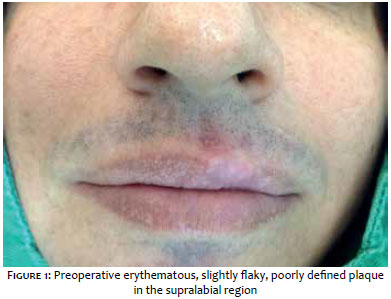
A 36 year-old male patient had had an erythematous infiltrated plaque in the central supralabial region for two years. The lesion's biopsy diagnosed Bowen's disease. He had undergone photodynamic therapy with methyl aminolevulinate (two sessions with an interval of one week), without resolution of the picture. The patient was then referred for Mohs micrographic surgery.
At the time of surgery, the lesion measured 1.5 x 0.9cm (Figure 1). Five stages were necessary for the total removal of the tumor, with histology compatible with Bowen's disease. The final defect measured 3.0 x 1.6cm (Figure 2). Eight units of botulinum toxin type A were then applied in the surgical wound, leaving to heal by secondary intention.
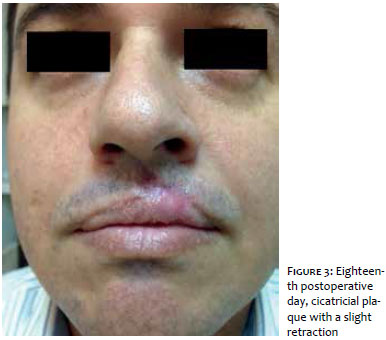
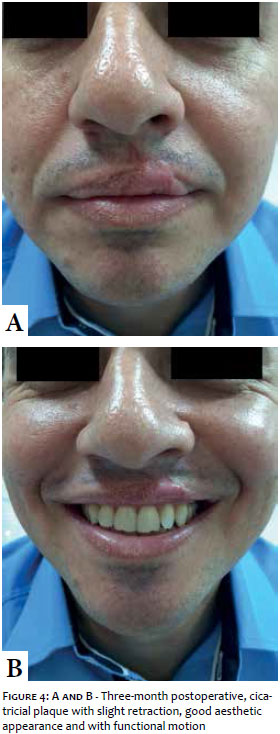
Eighteen days after the surgery there was complete healing of the wound, with the formation of a slightly erythematous cicatricial tissue in the upper lip and a discreet extension into the supralabial region (Figure 3). The resulting appearance remained in the late 3-month postoperative period, with excellent aesthetic and functional outcomes (Figure 4 A and B).
Botulinum toxin has been used to encourage the development of healing due to its immobilizer effect.6
In their study, Hei Sun et al. presented data in which the proliferation of fibroblasts – and consequently of type I collagen, the main component of the extracellular matrix – was significantly reduced after treatment with botulinum toxin type A due to its inhibitory action on the first. 3
Another finding presented in same study was the suppression of the differentiation of fibroblasts into myofibroblasts, which are responsible for the acceleration of the wound contraction process, by inhibiting the expression of TGF-β1. Myofibroblasts express the smooth muscle's alpha actin that is present in hypertrophic scars. 3 TGF-β1 expression is increased during abnormal scarring. By suppressing its expression, a reduction in the formation of pathological scarring is expected. 3
Analyses of reverse transcription reaction in polymerase chain demonstrated decreased levels of smooth muscle alpha-actin's mRNA in cells treated with TGF-β1 associated with botulinum toxin type A, when compared to cells treated only with TGF-β1. 3
Another study containing histological analysis noted that the weakening of the contraction effect might occur in the healing process when there is reduction of alpha-actin expression and myosin II in smooth muscles. The results also showed that
Another study containing histological analysis noted that the weakening of the contraction effect might occur in the healing process when there is reduction of alpha-actin expression and myosin II in smooth muscles. The results also showed that the higher the concentration of botulinum toxin type A, the more obvious the inhibition effect, thereby partially explaining the molecular mechanism for the toxin-based treatment. Thus, inhibiting fibroblast proliferation and reducing the expression of alpha-actin in smooth muscles and myosin II can determine the degree of fibrosis in a scar. 4
The botulinum toxin type A's molecular properties of suggest that their action is better at the beginning of healing, when the fibroblasts are still in the proliferative phase and intense apoptotic activity. 1 For this reason, many questions arise about the possible benefits of injection of botulinum toxin in surgical wounds, especially if applied intraoperatively, as was done with the patient treated in the present study.
Despite evidence of the significant contribution of botulinum toxin in promoting proper healing, possible benefits in the healing process by secondary intention were not yet evaluated. The successful outcome of the present case establishes a precedent for further studies on chronic ulcers, in addition to serving as a new alternative for reconstruction of surgical wounds.
1. Kim YS, Lee HJ, Cho SH, Lee JD, Kim HS. Early postoperative treatment of thyroidectomy scars using botulinum toxin: A split-scar, double-blind randomized controlled trial. Wound Rep Reg. 2014; 22(5): 605-12.
2. Mohammad M AQ, Bisher NAS, Feras A . Botulinum toxin type A: implications in wound healing, facial cutaneous scarring, and cleft lip repair. Ann Saudi Med. 2013; 33(5): 482-8.
3. Hii SJ, Byeong HL, Ha MS, Sook YP, Duk KA, Min SJ, et al. Effect of Botulinum Toxin Type A on Differentiation of Fibroblasts Derived from Scar Tissue. Plast Reconstr Surg. 2015; 136(2): 171e-78e.
4. Minliang C, Tongtong Y, Kui M, Linying L, Chang L, Liming L, et al. Botulinum Toxin Type A Inhibits - Smooth Muscle Actin and Myosin II Expression in Fibroblasts Derived From Scar Contracture. Ann Plast Surg. 2014 Aug 20. [Epub ahead of print]
5. Liu A, Moy RL, Ozog DM. Current Methods Employed in the Prevention and Minimization of Surgical Scars. Dermatol Surg. 2011;37(12):1740-6.
6. Freshwater MF. Botulinum toxin for scars: Can it work, does it work, is it worth it?. J Plast Reconstr Aesthet Surg. 2013; 66(3): e92-3.
This study was carried out at the Centro de Dermatologia, Cirurgia e Laser – Goiânia (GO), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}