


Raquel Zappa Silva Marques1; Daniela Kouvaleski Saviano Moran1; Carolina Speyer2; Luciana Cirillo Maluf Azevedo3; Simão Cohen4
Introduction: Rosacea is a chronic disease that usually manifests as flushing, persistent facial erythema, telangiectasia, papules and pustules. Intense Pulsed Light (IPL) is reported for treatment of vascular lesions of facial telangiectasia rosacea.
Objective: To assess clinical and dermoscopy improvement of facial erythema and flushing, and the clearing of vessels to dermoscopic after using IPL.
Methods: Nine patients were selected, with facial telangiectasic rosacea, aged between 36 and 59 years, with skin types I to III, without any treatment in the past six months. The treatment consisted in applications of the Intense Pulsed Light(IPL) with dual-band, 535-680 nm and 860-1200 nm, in one single shot. To favor the target hemoglobin, there is a greater protection for the skin. Three sessions were conducted within the interval of 1 month.
Results: After treatment, 87.5% of patients noticed reduction in flushing and telangiectasia. Adverse events were minimal and transient. To date no treatment was complete for telangiectasia rosacea.
Conclusions: This study demonstrated that treatment with IPL technology using "dual-band" is effective in obtaining a large (>75%) clinical improvement in 50% of patients and moderate improvement (51% to 75%) in 28.6% of patients.
Keywords: ROSACEAE; INTENSE PULSED LIGHT THERAPY; TELANGIECTASIA, ERYTHEMA
Rosacea is a chronic disease that usually manifests as flushing, persistent facial erythema, telangiectasia, papules and pustules. Intense Pulsed Light (IPL) is described for the treatment of vascular lesions of facial telangiectasic rosacea. 1
Intense Pulsed Light is a polychromatic, non-coherent light of broad electromagnetic spectrum, capable of emitting wavelengths between 390nm and 1,200nm.2
Its principle is based on the absorption of photons by endogenous or exogenous chromophores within the skin. This energy transfer to these target-chromophores generates heat and subsequent destruction of specific structures of the skin through a process called selective photothermolysis. The wavelength should be selected depending on the target-chromophore's peak absorption and the pulse's duration, which should be shorter than the thermal relaxation time. This limits the diffusion of heat and minimizes the damage to the surrounding structures. 3
The possibility of using different combinations of wavelength, pulse duration, time lapse between shots and fluences allows the use of IPL devices to treat various dermatological conditions, including rosacea.2
Rosacea is a chronic dermatosis of unknown etiology characterized by erythema, telangiectasia, papules and pustules.4, 5
In the present study, the authors used the Omnimax® platform (Sharp Light, Israel), which contains the IPL tip with double absorption band for hemoglobin (535-680 and 860-1,200nm).
Nine volunteers were selected (8 women and 1 man, aged between 36 and 59 years, with Fitzpatrick skin phototypes I-III). The following inclusion criteria were established: patients with telangiectasic rosacea (erythema, flushing, telangiectasias) without ambulatorial dermatological treatment for the previous six months. Exclusion criteria were: immunosuppression, neurological or immunological diseases, pregnancy, any local sign of infection or inflammatory skin disease, previous formation of hypertrophic scars or keloids, current use of aspirin or nonsteroidal anti-inflammatory, exposure to UV radiation in the previous four weeks and facial rejuvenation procedures (such as peels, acids, lasers or surgery) in the previous six months. The patients were recruited at the Dermatologic Clinic of the Faculdade de Medicina do ABC, with all having signed the free and informed term of consent. The study was approved by the Institution's Ethics Committee.
Photographs were taken at the beginning of each session and 30 days after the end of treatment, using a digital camera Nikon/Coolpix L320 equipped with ring flash attached to the lens (Lens-shift VR/16.1 megapixels). All photographs were taken in raw format under the same conditions and camera settings. Standardized points of view were used (facial at 90º, and right and left oblique at 45°).
Dermoscopic images were obtained before each session, without using flash, with special dermoscopic lenses (DermLite Hybrid, California, USA) attached to the Sony Cyber-Shot 14.1 megapixels Carl Zeiss lens, with the left medium pupillary line set at standardized 4cm below the lower eyelid, zoom at 3.3 and half of the intensity of the polarized dermoscope's light.
The used device was the Omnimax® (SharpLight, Israel), set on IPL, with two cut filters in the same shot (535-680nm and 860-1,200nm). The wave spectrum between 535 and 680nm primarily affects vascular lesions, and is well absorbed by melanin, meaning that it is also effective in the treatment of pigmented lesions. In turn, the spectrum between 860 and 1,200nm comprises intermediate levels of absorption by the melanin and hemoglobin, thus increasing its heating. Given that longer wavelengths penetrate deeper, this range is more effective for treating larger and deeper lesions. In the 680-860nm wavelength range, the laser shot does not act, increasing the epidermal protection due to the fact that the absorption of oxyhemoglobin and deoxyhemoglobin in this spectrum is relatively weak, even though melanin absorption is significant.
All patients were informed on the need for conducting three sessions with an interval of 30 days. Intense pulsed light was performed with fluences varying from 10 to 20 J/cm2, with pulse duration of between 12 and 25 ms, in one or two passes, depending on the severity of the clinical picture and the tolerance of each patient.
Prior topical anesthesia was not used in order to avoid constriction of the vessels. Patients were instructed to use sunscreen SPF 60 and oily lotion topically for protecting the skin between sessions of IPL.
Potential adverse effects, such as erythema, hypo and hyperpigmentation, blisters, purpura and scars were evaluated in each session using a scale to indicate the intensity of the alteration (none, mild, moderate or severe).
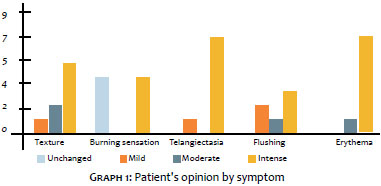
At the end of the study, a questionnaire was used to assess the treatment's efficacy using a scale based on the guidelines of the National Rosacea Society Expert Committee. 6 The symptoms evaluated were flushing, persistent erythema, telangiectasia, burning sensation and overall improvement of the skin. The ratings attributed ranged from 0 to 3 (0 - unchanged, 1 - mild, 2 - moderate, 3 - intense).
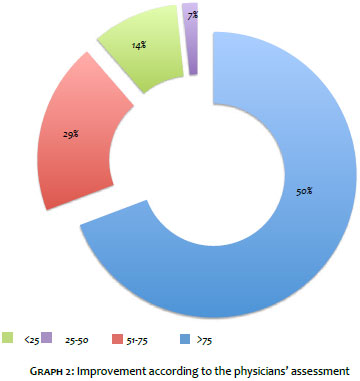
The before and after the treatment dermoscopic images were analyzed by two physicians, who observed the general development of the patients' clinical picture according to the following scale: <25%, 25-50%, 51-75% and above 75% improvement of the signs.
The study patients answered the questionnaire using a scale based on the guidelines of the National Rosacea Society Expert Committee, 6 in which a comparative assessment of the treatment's efficacy was carried out for the following variables: texture, burning sensation, telangiectasia, flushing and erythema.
The symptoms with most obvious improvements were erythema and telangiectasia, for which seven of the patients reported significant improvement. Opinions about the skin's texture and flushing were mostly positive, indicating there had been mild, moderate or intense improvement of the picture. Burning sensation was reported by 50% of patients (Graph 1).
Two physicians also individually evaluated the results through before and after the treatment photographs. The following scale was used: <25%, 25 to 50%, 51 to 75% and >75% improvement. In this analysis, the results were evaluated considering the general appearance of the patient, without differentiating the signals.
Of the analyzed cases, 50% were classified as having had more than 75% of improvement in the overall clinical picture, followed by the second highest improvement rating (51-75%), which has been achieved by 28.6% of patients who underwent treatment with IPL. Only 3 of the 14 analyzed photographs received ratings lower than 50% of clinical improvement (Figures 1 to 4) (Graph 2).
The results of only 8 patients were analyzed, as there was one desistance after the initial selection, due to pain and discomfort during the procedure.
A proven effective and safe treatment option for rosacea is the use of light-based technology. 1 The present study was based on the use of phototherapy with IPL operated within two light band ranges for facial rosacea in one single shot.
Intense pulsed light technology was designed to treat vascular and pigmented lesions, however it has other applications, such as hair removal and photorejuvenation. The fact that it can generate single or multiple synchronized pulses, coupled with the possibility of varying the duration of these shots, makes it a very versatile tool. 5
In the literature, Mark et al. 7 demonstrated reductions of 29% in telangiectasia and 21% in erythema after 5 sessions of IPL using a 515nm filter and single pulses with duration of 3ms. Similarly to what was done in the present study, Taub et al. performed a trial with approximately 500 patients, who underwent sessions of IPL or laser associated with bipolar radiofrequency. Based on medical evaluations, one month after the third sessions the patients had their erythema reduced to 1.21 from 2.38, and telangiectasia to 0.86 from 1.64 (maximum rating = 3). Moreover, they obtained an evident improvement in the skin's texture. 8 As compared to that trial, the present study yielded similar outcomes, with a significant improvement in symptoms of erythema, telangiectasia and in the skin's texture after the sessions.
With a smaller sample (34 patients), another article has demonstrated the efficacy of IPL. After 4 sessions, the erythema and severity scores, as well as the photographic evaluation improved significantly, with the results being maintained in a reassessment carried out six months after, with minimal and transient side effects. 5
In another study, the analysis of 60 patients bearers of telangiectasia associated with rosacea who underwent treatment with IPL using a wide wavelength spectrum (ranging from 515 to 1,200nm) and different filters (515, 550, 570 and 590nm) during a period of approximately 2 years, it was possible to observe improvement in 77.8% of the lesions. 9
The present evaluation showed that the IPL treatment was effective in obtaining intense improvement (>75%) in the clinical aspect of 50% of patients, and moderate improvement (51-75%) in 28.6% of patients, with minimal and transient side effects.
Treatment with IPL increases the amount of superficial collagen and elastic fibers in the dermis. This is due to the selective absorption of light by the water contents in the tissues, increasing the conduction of heat around the collagen, therefore increasing its production. Furthermore, there is increased production of fibroblasts by the photothermal effect. This mechanism explains the better results reported by patients younger than 40, as evidenced by Lim et al. 1
By using this laser type, it is possible to destroy abnormal blood vessels, reduce the inflammation and the number of active sebaceous glands, in addition to block the altered keratinization process. All these effects contribute to the overall improvement of the rosacea's clinical picture. 8
1. Lim HS, Lee S-C, Won YH, Lee J-B. The Efficacy of Intense Pulsed Light for Treating Erythematotelangiectatic Rosacea Is Related to Severity and Age. Ann Dermatol. 2014; 26(4): 491-45.
2. Ciocon DH, Boker A, Goldberg DJ. Intense pulsed light: what works, what's new, what's next. Facial Plast Surg. 2009; 25(5): 290-300.
3. Piccolo D, Di Marcantonio D, Crisman G, Cannarozzo G, Sannino M, Chiricozzi A, et al. Unconventional Use of Intense Pulsed Light. Biomed Res Int. 2014;2014:618206.
4. Babilas P, Schreml S, Szeimies R, Landthaler M. Intense pulsed light (IPL): a review. Lasers Surg Med. 2010; 42(2): 93-104.
5. Papageorgiou P, Clayton W, Norwood S, Chopra S, Rustin M. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol. 2008;159(3):628-32.
6. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, et al. Standard classification of rosacea: Report of the National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584-7.
7. Mark KA, Sparacio RM, Voigt A, Marenus K, Sarnoff DS. Objective and quantitative improvement of rosacea-associated erythema after intense pulsed light treatment. Dermatol Surg. 2003;29(6):600-4.
8. Taub AF. Treatment of rosacea with intense pulsed light. J Drugs Dermatol. 2003;2(3):254-9.
9. Schroeter CA, Haaf-von Below S, Neumann HAM. Effective treatment of rosacea using intense pulsed light systems. Dermatol Surg. 2005;31(10):1285-9.
This study was carried out at the Faculdade de Medicina do ABC (FMABC) – Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}