


Fabíola Rosa Picosse1; Danielle Cristine Bonatto2; Karime Marques Hassun3; Sérgio Talarico Filho4; David Rubem Azulay5; Ediléia Bagatin6
Introduction: Acne vulgaris is a chronic inflammatory disease of the pilosebaceous follicles. Treatment should be early and effective to prevent scarring and psychosocial effects, and isotretinoin is the drug of choice for moderate or severe cases.
Objective: To assess efficacy, safety and tolerability of an isotretinoin similar to the reference product.
Methods: A bicentric study, with therapeutic intervention was conducted, including 50 participants aged 13 to 35 years, with moderate to severe acne, using isotretinoin 0.5 mg/kg/day up to 120 mg/kg. Efficacy was assessed through lesions counting, the investigator's global assessment (IGA) scale, patient satisfaction and application of the quality of life questionnaire specific for Acne (Acne Qol). Safety and tolerability were assessed by analysis of adverse events and laboratory tests. Results: Mean age was 20 years, 70% of participants were men, with a reduction of 99% of lesions after treatment and complete remission of lesions in 91.5% of participants. IGA scale reduced 98% in the score after treatment. Also, 100% of participants declared to be satisfied, with significant improvement in quality of life. Adverse events were similar to those described in the literature.
Conclusion: The assessed isotretinoin was equally effective, safe and well-tolerated when compared with published data of the standard product.
Keywords: ACNE VULGARIS; TREATMENT OUTCOME; ISOTRETINOIN
Acne vulgaris is a chronic inflammatory dermatosis of the pilosebaceous follicles. It is considerably common and affects a percentage that ranges from 79% to 95% of the adolescent population in Western societies. The condition was also reported in 8% of adults between 25 and 34 years of age and in 3% of those between 35 and 44 years old. 1, 2
Its pathogenesis is multifactorial and results in the occlusion of the sebaceous follicles due to the excessive amount of sebum produced by the sebaceous glands, which stimulation is mediated by androgens, combined with hyperkeratinization and excessive desquamation of epithelial cells in the follicles' walls. This occlusion leads to formation of a micro comedo, which is considered as the primary lesion of acne, and that can become a comedo or an inflammatory lesion. The proliferation of the Propionibacterium acnes bacteria is also one of the factors that contribute to the pathogenesis of acne and is favored by an environment created by the mixture of sebum and follicular cells. In addition, this bacterium is responsible for the release of chemotactic factors, such as cytokines and tumor necrosis factor (TNF), which initially attract neutrophils and mast cells, which in turn lead to inflammation. 3-5 The P. acnes modulates the expression of the toll-like receptor 2 (TLR-2), activating several nuclear pathways such as NFKB, with the production of other proinflammatory cytokines and the AP-1 pathway, which determines the production of metalloproteinase enzymes, implicated in the development of acne scars. Qualitative changes in sebum secretion are also involved in the inflammation that has been regarded as the central event in acne – present even before the onset of clinical inflammatory lesions such as papules, pustules and nodules. 6, 7 In addition to these mechanisms, genetic factors, stress among others, influence the development and severity of acne.
It is clinically classified as non-inflammatory or comedonian (presence of open and closed comedones) and inflammatory (characterized by papules, pustules, nodules, cysts and abscesses). Inflammatory acne can be sub-divided into mild, moderate and severe. All lesions can leave scars of various types. 8
Treating the acne is of utmost importance to reduce its severity, potential for recurrence, scarring and psychosocial impact, contributing to improved quality of life. Topical treatments (retinoids, benzoyl peroxide, antibiotics, azelaic acid) are recommended for comedonian and mild to moderate inflammatory acne. For moderate to severe cases, treatment should be carried out with a combination of topical and/or systemic drugs (antibiotics, hormones), since it is a multifactorial disease. 9-11 Isotretinoin, a retinoid derivative of vitamin A, is widely used to treat acne as a monotherapy, since it is the only substance capable of controlling all etiopathogenic factors. 12 Retinoids act in the growth and differentiation of epidermal cells, and the isotretinoin interferes with the activity of the sebaceous gland, has immunomodulatory and anti-inflammatory properties, modulating the TLR 2's activity. As a result, there are a decrease in the comedogenesis, a reduction in the size of the sebaceous glands greater than 90% due to a decreased basal proliferation of sebocytes, a suppression of sebum production and the inhibition of the differentiation of the terminal sebocyte. Although it does not directly affect Propionibacterium acnes, the reduction of sebum alters the follicular microenvironment, reducing the number of bacteria and their ability to cause inflammation. It has already been shown that oral isotretinoin significantly reduces the population of P. acnes resistant to three antibiotics: erythromycin, clindamycin and tetracycline. 13, 14
Oral isotretinoin was synthesized in 1955, however only in 1973 the studies on its clinical use in psoriasis began, giving rise to further evaluation on its use in other keratinization disorders.15 By 1976, it started to be tested in Europe for the treatment of acne. In 1978, a study showed its excellent effect on nodule-cystic acne, with complete and prolonged remission. 16 In the following year, positive outcomes were reported in 14 patients treated with 2mg/kg/day for four months.17 In 1980, similar results were obtained with the daily dose of 0.1 to 1mg/kg over four months. 18 Only in 1982, however, the first double-blind, randomized study was published, effectively demonstrating the efficacy of oral isotretinoin with a maximum daily dose of 1.2 mg/kg for four months in 33 patients bearing severe forms of acne.19
The approved indications for oral isotretinoin are: nodular-cystic acne and pustular papular acne resistant to other treatments or with frequent improvements and recurrences.20-22 The daily dose is calculated according to the patient's weight and ranges from 0.5 to 1 mg/kg. 23, 24 In order to prevent recurrences, a total dose of between 120 and 150mg/kg is recommended.
Adverse reactions to isotretinoin can be divided into two types: a) undesirable, predictable and controllable pharmacological effects (cutaneous-mucosal) and b) toxic effects involving organs and systems, when no therapeutic effect is expected, particularly alterations in liver function and in serum lipids.25-28 It is important to advise the patient on the cutaneous-mucosal effects, to prevent and treat early, with the use of lip lubricant and hydrating the skin and nasal and conjunctival mucosas, and use sunscreen daily aimed at preventing that these adverse events become the unnecessary cause for the interruption of treatment. Similarly, laboratory monitoring is required. Teratogenicity is the most serious risk, and the patient must wait for the menstruation to start the treatment and be guided regarding contraception, with two safe methods, during and up to one month after the end of the treatment. 29-31
Several pharmaceutical companies manufacture this drug, with a frequent doubt among patients, and even dermatologists, being whether the similar isotretinoin has the same efficacy and safety of the standard product.
In this manner, the objective of the present study was to evaluate the efficacy, safety and tolerability of a similar isotretinoin as compared to the standard isotretinoin.
A bicentric, therapeutic intervention, open and uncontrolled study was carried out to evaluate the efficacy, safety and tolerability of oral isotretinoin contained in gel capsules (Acnova®) produced by the pharmaceutical company Germed Pharma Ltda. (Campinas, SP, Brazil), in patients with moderate to severe acne vulgaris.
With the approval by the Research Ethics Committee (07527912.7.1001.5505), all participants signed the Free and Informed Term of Consent. Observing the inclusion and exclusion criteria, 50 patients were selected: 25 in each center, of both genders, aged between 13 and 35 years, with clinical diagnosis of moderate to severe facial acne, who used the studied drug orally (gel capsules) once or twice a day, with individual dose adjustment (~ 0.5mg/kg body weight/day) up until the total dose of 120mg/kg for up to 12 months.
Patients were followed up in eight visits, with clinical, laboratory and photographic assessments.
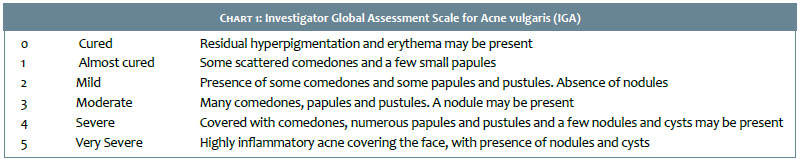
The impact of the treatment on the patients' quality of life was evaluated through an acne specific questionnaire (Acne QoL) before and after the treatment. The efficacy was assessed by the lesion counts (total, inflammatory and non-inflammatory), change in the intensity/severity of acne according to the Investigator Global Assessment (IGA) (Chart 1) and the patient's satisfaction. The outcomes were analyzed applying the negative binomial regression method for panel data (longitudinal data) using the Stata/SE 13.1 software's xtnbreg procedure (Stata Corp, CollegeStation, Texas), as well as the comparison of the Acne QoL's scores before and after the treatment, through the linear regression analysis for panel data using the xtreg procedure (Stata Corp). The safety and tolerability were assessed by observation and based on reports of adverse events during the follow-up and laboratory tests, through linear regression analysis for panel data using the xtreg procedure (StataCorp). The results are presented as risk ratios (RR) and oddsratio (OR).
A significance level of 5% (α = 0.05) was adopted throughout the analysis, meaning the results were considered significant when the p-value was less than 5% (p <0.05).
The age of the 50 participants ranged from 13 to 35 years old, with a mean of 20 years old. Seventy percent were men.
There were 3 premature withdrawals due to personal reasons (not for adverse events), meaning that 47 patients completed the treatment, with 41 (87.2%) becoming very satisfied and 6 (12.8%) satisfied with the outcome.
For purposes of analysis 3 visits considered (initial, intermediate and final). The average time elapsed between the initial and intermediate visits was 118 days or roughly 4 months (standard deviation = 14 days). The average time elapsed between initial and the final visits was 249 days or roughly 8 months (standard deviation = 51 days).
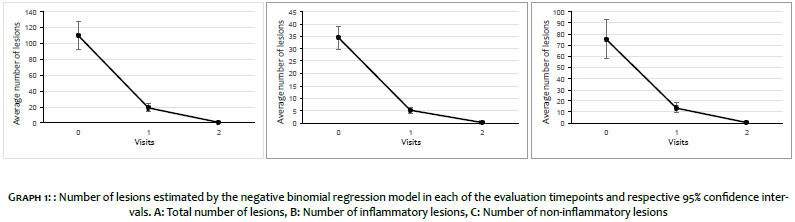
Regarding the number of lesions when compared to the initial visit, the following facts were observed: mean reduction of 83% in the estimated total number of lesions in the intermediate visit, and of 99% at the final visit (p <0.001). For the inflammatory lesions, the reductions were 85% and 99%, and for the non-inflammatory, 82% and 99%, respectively (p <0.001), as depicted in Graph 1.
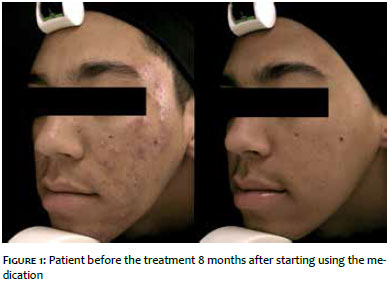
The total remission of the lesions was observed in 91.5% of participants, as shown in Figures 1 and 2.
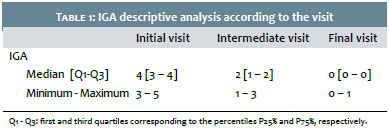
Analyzing the intensity/severity of acne according to the IGA Scale regarding the initial visit, an estimated average reduction of 50% was verified in the intermediate visit (CI 95%: 45%; 56%). The estimated average reduction in the final visit was 98% (CI 95%: 94%; 99%), with p <0.001, as shown in Table 1.
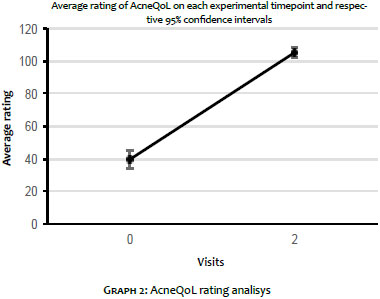
The analysis of the impact of the treatment on the participants' quality of life evidenced that the mean score arising from the Acne QoL questionnaire was 39.5 + 19.4 before the treatment and 105.1 + 10.0 at its end. Using the regression model for panel data it was possible to conclude that this increase was significant (p <0.001), having been estimated at 65.5 points (CI 95%: 59.5; 71.7), suggesting the presence of a significant improvement in the patients' quality of life (Graph 2).
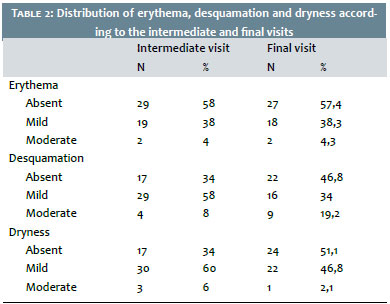
Safety and tolerability were assessed in the intermediate and final visits by assessing the presence of erythema, desquamation and skin dryness. Table 2 shows the distribution of these occurrences. It is possible to note that in the intermediate visit 42% of patients had erythema, 66% had desquamation, and 66% had dryness. At the final visit, 42.6% had erythema, 53.2% had scaling, and 48.9% had dryness.
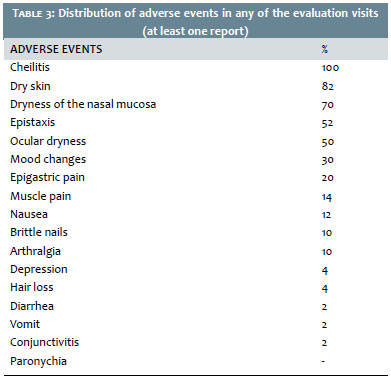
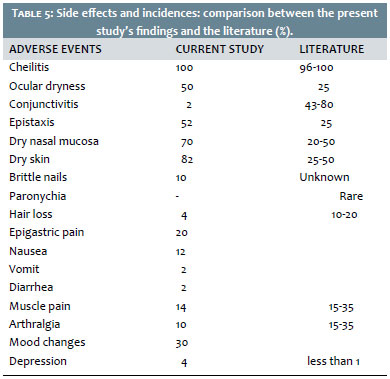
Throughout the evaluation, patients were asked about the presence of other adverse events. Table 3 shows the distribution of these adverse events (with at least one occurrence, at any time during the study). No serious adverse event was observed.
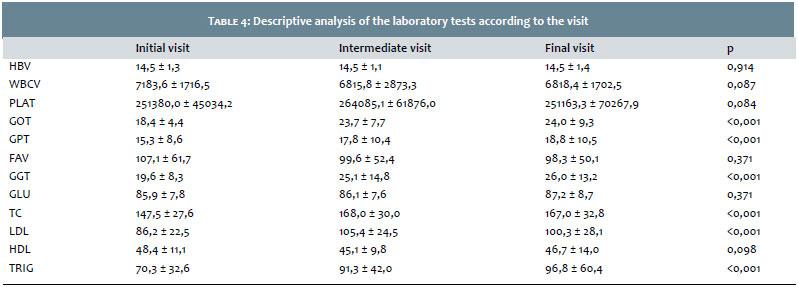
Table 4 presents the analysis of laboratory tests.
It was possible to observe that GOT, GPT, gamma GT, total cholesterol, LDL and triglycerides varied along the study period, nevertheless their mean values did not exceeded or fell below reference values. There was no need to discontinue the treatment due to laboratory abnormalities. Blood count, alkaline phosphatase, glucose and HDL did not change significantly.
The efficacy of oral isotretinoin in the treatment of acne vulgaris has been demonstrated in numerous publications since the 80s, with more than 90% of reduction of inflammatory lesions. In the present study, the authors observed a 99% reduction of inflammatory and non-inflammatory lesions, with 100% satisfaction of participants and significant improvement in the quality of life.31
The treatment duration (roughly 6 months), is described as sufficient for acne remission in 99% of patients. In the present study, the average duration of treatment was eight months.32
As a rule, it is expected a 50% reduction of the pustules within 2 to 4 weeks after the beginning of the treatment. The authors of the present study observed a reduction of 85% in inflammatory lesions in the 4th month of treatment and, in line with the literature, inflammatory lesions improved faster than the comedones. Pustules receded before papules and nodules.31, 32
Regarding the alterations found in laboratory tests, there is great variability among studies, depending on the dose used. The most commonly found in the literature are elevated hepatic enzymes (20%), increased triglycerides (20-40%), and increased serum cholesterol with elevated LDL fraction and decreased HDL (10-30%), in line with the present study's observations, even in light of the fact that the mean values remained within the reference levels used in the laboratory. There are reports of hepatotoxic reactions in less than 1% of cases, which was not observed in the present study.31, 32
Thus, it is possible to assert that the studied similar isotretinoin led to outcomes similar to those found in the literature for the standard isotretinoin regarding its efficacy, safety and tolerability.
The present study is of great practical applicability in the dermatologist's daily life, for the equivalence of similar and standard isotretinoins regarding their safety and effectiveness is often a source of doubt for both patients and even dermatologists.
Limitations of the present study include: the small number of participants and the study design (open, non-controlled or comparative and non randomized).
Despite the limitations of the present study, it was possible to conclude that the evaluated similar isotretinoin was equally effective, safe and well tolerated when compared to the literature data on the standard product, a fact that adds great value to the dermatologist's daily routine.
1. Cardain LG, Lindeberg S, Hurtado M, Hill K, Eaton SB, Brand-Miller J. Acne Vulgaris - A disease of western civilization. Arch Dermatol. 2002;138(12):1584-90.
2. Dréno B, Khammari A. Acne – inflammatory affection of pilosebaceus follicle: the most frequent cutaneous illness of moderne time. In: European PharmacoTherapy 2003 – September 2003. London: Business briefing Ltd; 2003. p.130
3. Gollnick H. Current Concepts of Pathogenesis of Acne - Implications for Drug Treatment . Drugs. 2003;63(15):1579-96.
4. Harper JC, Thiboutot DM. Pathogenesis of acne: recent research advances. Adv Dermatol. 2003;19:1-10.
5. Koreck A, Pivarcsi A, Dobozy A, Kemény L. The role of innate immunity in the pathogenesis of acne. Dermatology. 2003;206(2):96-105.
6. Mclnturff JE, Modlin RL, Kim J. The role of toll-like receptors in the pathogenesis and treatment of dermatological disease. J Invest Dermatol. 2005; 125(1):1-8.
7. Rocha MA, Costa CS, Bagatin E. Acne vulgaris: an inflammatory disease even before the onset of clinical lesions. Inflamm Allergy Drug Targets. 2014; 13(3):162-7.
8. Pochi PE, Shalita AR, Strauss JS, Webster SB, Cunliffe WJ, Katz HI, et al. Report of the consensus conference on Acne classification. J Am Acad Dermatol. 1991; 24(3):495-500.
9. Gollnick H, Cunliffe WJ, Berson D, Dréno B, Finlay A, Leyden JJ, et al. Management of acne: a report from a global alliance to improve outcomes in acne. J Am Acad Dermatol. 2003; 49(1 suppl) :S1-38.
10. Sampaio SAP, Bagatin E. Experiência de 65 anos no tratamento da acne e de 26 anos com isotretinoína oral. An Bras Dermatol. 2008; 83(4):361-7.
11. Strauss JS, Krowchuk DP, Leyden JJ. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007; 56(4):651-63.
12. Hassun KM. Etiopatogenia da acne. An Bras Dermatol. 2000; 75(1):7-15.
13. Layton AM, Knaggs H, Taylor J, Cunliffe WJ. Isotretinoin for acne vulgaris - 10 years later: a safe and successful treatment. Br J Dermatol.1993; 129(3):292-6.
14. Coates P, Adams CA, Cunliffe WJ, McGinley KT, Eady EA, Leyden JJ, et al. Does oral isotretinoin prevent Propionibacterium acnes resistance? Dermatology. 1997; 195(Suppl 1):4-9.
15. Ginsberg H, Rubenstein A, Brown WV. Medical complications of isotretinoin. Clin Dermatol. 1986; 4(1):183-9.
16. Peck GL, Yoder FW, Olsen TG, Pandya MD, Butkus D. Treatment of Darier's disease, lamellar ichthyosis, pityriasis rubra pilaris, cystic acne and basal cell carcinoma with oral 13 cis retinoic acid. Dermatologica. 1978; 137 (Suppl 1):11-2.
17. Peck GL, Olsen TG, Yoder FW, Strauss JS, Downing DT, Pandya M, et al. Prolonged remission of cystic acne and conglobate acne with 13 cis retinoic acid. N Engl J Med. 1979; 300(7):329-33.
18. Jones H, Blanc D, Cunliffe WJ. 13-cis retinoic acid and acne. Lancet. 1980; 2(8203):1048-9.
19. Peck GL, Olsen TG, Butkus D, Pandya M, Arnaud-Battandier J, Gross EG, et al. Isotretinoin versus placebo in the treatment of cystic acné. A randomized double-blind study. J Am Acad Dermatol. 1982;6(4 Pt 2 Suppl):735-45.
20. Leyden JJ. Oral isotretinoin. How can we treat difficult acne patients? Dermatology. 1997; 195(Suppl 1):29-33.
21. Farrell LN, Strauss JS, Stranieri AM. The treatment of severe cystic acne with 13-cis-retinoic acid. Evaluation of sebum production and the clinical response in a multiple-dosis trial. J Am Acad Dermatol. 1980; 3(6):602-11.
22. Herane Herane MI. Nuevas pautas de uso de isotretinoína oral en acné. Dermatología (Santiago de Chile). 1994; 10:138-9.
23. Corlin R, Maas B, Mack HA. Oral administration of low dosis of 13-cis-retinoic acid in papulopustular acne. Results of a multicenter study. Hautarzt. 1984; 35(12):623-9.
24. Strauss JS, Rapini RP, Shalita AR, Konecky E, Pochi PE, Comite H, et al. Isotretinoin therapy for acné: results of a multicenter dosis-response study. J Am Acad Dermatol. 1984; 10(3):490-6
25. Saurat JH. Side effects of systemic retinoids and their clinical management. J Am Acad Dermatol. 1992; 27(6 pt 2):523-8.
26. Charakida A, Mouser PE, Chu AC. Safety and side effects of the acne drug, oral isotretinoin. Expert Opin Drug Saf. 2004; 3(2):119-29
27. Almeida ADT, Santos FLF, Santana DP. Isotretinoína e seus efeitos clínicos tóxicos. Rev Farm Bioquim Univ São Paulo. 1998; 34(2):41-6.
28. Koistinen HA, Remitz A, Gylling H, Miettinen TA, Koivisto VA, Ebeling P. Dyslipidemia and a reversible decrease in insulin sensitivite induced by therapy with 13-cis-retinoic acid. Diabetes Metab Res Ver. 2001; 17(5):391-5
29. Chan A, Hanna M, Abbott M, Keane RJ. Oral retinoids and pregnancy. Med J Aust. 1996; 165(3):164-7.
30. Thiboutot D, Gollnick H. New insights into management of acne: an update from the Global Alliance to improve outcomes in acne group. J Am Acad Dermatol. 2009; 60(5 Suppl):S1-50.
31. McLane J. Analysis of common side effects of isotretinoin. J Am Acad Dermatol. 2001; 45(5):S188-94.
32. Ellis CN, Krach KJ. Uses and complications of isotretinoin therapy. J Am Acad Dermatol. 2001; 45(5):S150-7.
33. Goulden V, Layton AM, Cunliffe WJ. Long-term safety of isotretinoin as a treatment for acne vulgaris. Br J Dermatol. 1994; 131(3):360-3.
This study was carried out at the Medical School of the Universidade Federal de São Paulo (UNIFESP) - São Paulo (SP), Brazil and the at the Instituto de Dermatologia Professor Rubem David Azulay da Santa Casa de Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}