


Agnes Mayumi Nakano Oliveira1; Ivander Bastazini Júnior2; Tatiana Cristina Pedro Cordeiro de Andrade3; Cleverson Teixeira Soares4
Introduction: Glomus tumor is a benign and rare neoplasm that appears as solitary and painful nodule, mainly subungual. It presents characteristic clinical manifestations such as paroxysmal pain and sensitivity to local pressure and to cold.
Objective: To conduct a clinical epidemiological survey of glomus tumors diagnosed in a reference unit in 16 years.
Methods: Retrospective study assessing clinical and epidemiological data of 15 patients with glomus tumor confirmed by histopathological report from 2000 to 2016. Data on age, gender, tumor location, associated symptoms, duration of symptoms until diagnosis, clinical presentation, histological type and recurrence after surgery were analysed.
Results: Fifteen cases were diagnosed, 11 in women (73.3%) and four in men (26.7%). Mean age was 63 years. The most frequent location was the subungual region. Mean duration of symptoms until diagnosis was 8 years.
Conclusions: In this study, the number of cases of glomus tumor fluctuated throughout these 16 years, with a mean of 0.9 cases/year. A higher prevalence in women over 60 years, subungual region location and solid glomus histologic subtype was observed.
Keywords: GLOMUS TUMOR; NAIL DISEASES; NEOPLASMS
The glomus body is a highly specialized arteriovenous anastomosis responsible for thermoregulation.1 It is located in the reticular dermis throughout the body, and is present in high concentrations in the digital extremities, especially underneath the nail.2 As a result, the most common location of the tumor is the hands (75% of cases), with preference for the fingertips and subungual space. Other body sites, such as central nervous system, stomach, liver, mediastinum, trachea, lungs, bones, joints and genitals have been mentioned in the literature. Glomus tumor is a benign hamartoma of the glomus body, 1 corresponding to 1 - 4.5% of tumors of the hand. 3, 4, It was first described in 1812 by Wood as a very painful subcutaneous tumor with slow growth and sensitive to temperature variations. 2, 4 It emerges as an intensely sensitive (in special to cold), small, purple or bluish nodule, painful to the touch. 1, 4 Multiple locations are uncommon and mainly occur in children under 16 years old. 2 Solitary tumors are usually found in adults with usually between 30 and 50 years of age, with subungual location, predominantly in females.1-4 Solitary or multiple tumors have been described in association with neurofibromatosis type 1.1 Congenital and hereditary forms have autosomal dominant inheritance.3 The tumor occurs by hyperplasia in one or more normal parts of the glomus body. 2 The pain develops from the contraction of glomus cells.2 Clinical occurrences are hyperesthesia and/or localized paroxysmal pain, which increase with exposure to cold. 2 Hypersensitivity to cold is observed in 63 to 100% of cases located in the hands, however it is rarely found in extradigital tumors. The combination of magnetic resonance imaging, clinical tests and histopathology allows the diagnosis.2 There are three main clinical tests for the diagnosis of this tumor. 2, 4 The first is the Love's pin test, when the area where the pain is located is gently pressed with the tip of a pin or clip; in subungual tumors the pressure is directed to the nail plate at different locations until the exact area of the sensitivity is determined.2, 4 For a positive test, the patient should feel intense pain, sometimes with the jerking of the hand.2 The Hildreth's test involves placing a tourniquet on the base of the finger where the tumor is located, subsequently applying the Love's test.2, 4 For a positive result, the patient should not feel pain.2, 4 The third test is that of the sensitivity to the cold, which is expected to produce increased pain with exposure to cold. 2
Combined with the clinical tests, high-resolution imaging, such as magnetic resonance, has provided a valuable method for the diagnosis of the glomus tumor. Most of these tumors show high signal intensity on T2 and intense enhancement after gadolinium injection.2 Plain radiography may evidence bone erosion, suggesting the diagnosis, nevertheless it is a rare finding and takes place in only 22% of cases.3, 4 Other tests have been described, however with little contribution to the diagnosis. 4
Histologic analysis of the glomus tumor characterizes it with the presence of small vessels with normal endothelium, circumscribed by compact nests of polygonal cells with round and central nuclei, and eosinophilic cytoplasm. 5 Seven distinct histological forms are described. The glomangioma, which is the most common variant, has a prominent vascular component, with the vessels' lumen being dilated or cavernous. Some cases can have hyalinization of the vessels' walls and thrombi within them. The glomangiomyoma is a rare type, being characterized by muscle cells increased in size and number, surrounding the vascular spaces. The other described types of glomus tumors are: solid, symplastic, glomangiomatosis, infiltrate and malignant. 5 In most cases, surgical treatment leads to the complete resolution of symptoms.1, 3 Recurrence after surgery occurs in 4 to 15% of cases, depending on the series.1 Malignant transformation is rare (less than 1% of cases of glomus tumors) and occurs most commonly in non-acral locations. 6
The objective of the present study was to perform a clinical epidemiological survey of glomus tumors diagnosed at a reference unit during a period of 16 years.
A retrospective review of medical records of patients diagnosed with glomus tumor was carried out at the Dermatology Division of the Instituto Lauro de Sousa Lima, in the city of Bauru (São Paulo, Brazil), covering a 16-year period (from 01/01/2000 to 01/01/2016). The following variables were analyzed: age, gender, tumor location, associated symptoms, duration of symptoms up until diagnosis, clinical appearance, histological type and recurrence after surgery.
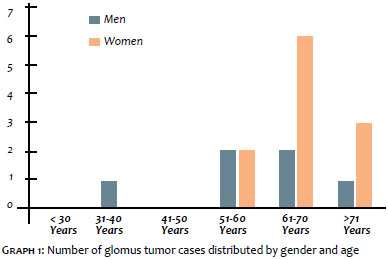
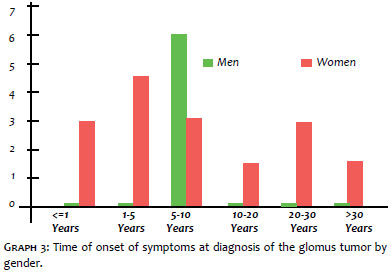
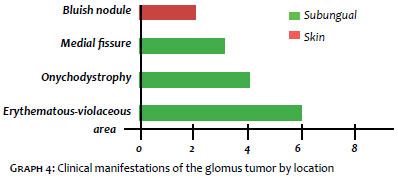
Between the years of 2000 and 2016, 15 cases of glomus tumor were diagnosed (11 women = 73.3% and 4 men = 26.7%, all Caucasian) (Graph 1). The average age at diagnosis was 63 years (min = 36, max = 85), with a predominance of the 61 to 70 years old age group (40%). The average age of women was slightly higher than that of men (66 and 54, respectively). Regarding the location of the lesion, the most common topography was the subungual in the fingers (60%), followed by the hallux (20%), dorsum (6.8%), lower limbs (6.7%) and arms (6.7 %). In both genders the glomus tumor occurred preferably in the subungual region (men = 50%, women = 73%) (Graph 2). The average time of onset of symptoms at diagnosis was 8 years (min = 1, max = 30) (Graph 3). Clinical abnormalities most frequently found were: erythematous-violet dotted area visualized through the nail plate (40%); onychodystrophy (26.7%); medial fissure in the nail plate (20%); and painful bluish nodule in the skin (13.3%) (Graph 4). Pain was present in 100% of patients. The most common histological type was the solid glomus tumor (86.7%), followed by glomangiomas (13.3%). Regarding the treatment, all patients underwent surgical excision, with 13.3% presenting recurrence.
In the present study, the number of diagnosed cases of glomus tumor fluctuated throughout the study period, with a mean value of 0.9 case/year. Regarding the topography, the most common site was the subungual region of the upper limbs (60%), followed by the hallux (20%), dorsum (6.8%), legs (6.7%) and arms (6.7%). The average time to diagnosis was 8 years. Unlike the present study, a review performed by the Mayo Clinic with 56 extradigital cases evidenced prevalence in the forearms (20%) and knees (18%). 7
A higher prevalence of glomus tumor was observed in women over 60 years of age and in the subungual region of the upper limbs. These data are in line with the literature, nonetheless differing in age, with the present study evidencing cases at an older age group. 3, 4
The most frequently found histological subtype was the solid glomus tumor (86.7%), a fact that did not corroborate findings of previous studies, which suggest the glomangioma as the most frequent. 5 The most often observed clinical appearance of the subungual glomus tumor was an erythematous-violaceous area (40%). The clinical tests, useful due to their easy implementation and cost effectiveness, have been performed only in 2 of the 15 cases (13.3%), yielding positive results in both.
Imaging studies were performed in 6 cases (40%), with plain radiography being performed in 4 of them. In only 1 case focal osteolysis was observed in the distal phalanx (25%). Magnetic resonance imaging was performed in 1 case, evidencing the tumor and its topography, leaving no doubt as to the diagnosis. Ultrasonography was requested in 1 case, however it did not evidence injury.
The found recurrence rate was 13.3%, coinciding with that in the literature. 3, 4
The present study has demonstrated that the glomus tumor is associated to a delay in its diagnosis, leading the patient to live with chronic pain and which most often has excellent response to surgical treatment. Although this entity is more often found in the subungual region, it can emerge in other body sites. In addition, specific clinical tests are excellent, cost-effective tools when there is suspicion of the diagnosis.
1. Willard KJ, Cappel MA, Kozin SH, Abzug JM. Benign Subungual Tumors. J Hand Surg Am. 2012;37(6):1276-86; quiz 1286.
2. McDermott EM, Weiss APC. Glomus Tumors. J Hand Surg. 2006; 31(8):1397-400.
3. Cernea SS, Di Chiacchio N, Vanti A. Tumores glômicos subungueais tratados pela cirurgia micrográfica de Mohs: índices de recidiva e revisão de literatura. Surg Cosmet Dermatol. 2009;1(2):70-3.
4. Vanti AA, Cucé LC, Di Chiacchio N. Tumor glômico subungueal: estudo epidemiológico e retrospectivo, no período de 1991 a 2003. An Bras Dermatol. 2007;82(5):425-31.
5. Calonje E, Brenn T, Lazar A. Mckee, PH. McKee's Pathology of the skin. 4th. ed. British Library: Connective tissue tumors. 2011. p. 1746-49.
6. Lancerotto, L.; Salmaso, R.; Sartore, L.; Bassetto, F. Malignant Glomus Tumor of the leg Developed in the Context of a Superficial Typical Glomus Tumor. Int J Surg Pathol. 2012; 20(4): 420-24.
7. Schiefer TK, Parker WL, Anankwenze AO, Amadio PC, Inwards CY, Spinner RJ. Extradigital glomus tumors: a 20 years experience. Mayo Cli Proc, 2006; 81(10): 1337-44.
This study was carried out at the Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}