


Kelly Cristina Signor1; Denise Steiner2; Dirlene Roth3; Miguel Luiz Batista Júnior4; Luciana Gasques de Souza5; Kaltinaitis Benetton Nunes Hypolito dos Santos6
Introduction: Stromal vascular fraction derived from adipose tissue is a rich source of different cells, containing large amounts of stem cells, which ability for diferentiation into various strains. In dermatology, there are several studies on the effectiveness of stem cells, which present antioxidant and rejuvenating effects. However, there are few reports about the anti-aging effects of stromal vascular fraction.
Objective: To evaluate the effectiveness of stromal vascular fraction in facial rejuvenation.
Methods: A prospective, comparative, controlled study was carried out, wit, with 10 patients divided into two groups and subjected to treatment of nasolabial folds with: Group 1: stromal vascular fraction and Group 2: conventional filler (calcium hydroxyapatite). Clinical, photographic and histological evaluations were conducted, with statistical analysis of data.
Results: Both techniques produced satisfactory results and were similar.
Conclusion: Application of stromal vascular fraction is a relatively new technique that presents good clinical results and is a promising option for rejuvenation.
Keywords: ADULT STEM CELLS; SKIN AGING; REJUVENATION
Adult stem cells have been the subject of many studies due to the absence of both ethical issues that embryonic stem cells may arise and their carcinogenic potential. Among adult stem cells, staminal cells derived from adipose tissue (adipose-derived stem cells - ADSCs) essentially have the same properties of stem cells derived from bone marrow.1 In addition, they have the advantages of being more accessible and relatively more abundant as compared to other types of adult stem cells. Experiments using ADSCs have been conducted more often in recent years. In dermatology, there are several studies on the effective application of stem cells – for instance on their antioxidant action and rejuvenating effects.2-4 Among the facts described in the latest publications, the ADSC's effects in the healing of wounds stand out, as well as their role in the photodamaged and aged skin. 5
The adipose tissue's stromal vascular fraction (SVF) is a source rich in preadipocytes, mesenchymal stem cells, endothelial progenitor cells, T and B cells, monocytes, macrophages and fibroblasts. Due to the fact that it contains a large population of adipose tissue-derived stem cells, it is able to differentiate into diverse lineages. 6, 7
Skin aging involves a series of different degenerative processes as well as a significant decrease in collagen produced by fibroblasts. Several cytokines and growth factors are also involved, stimulating the synthesis of collagen by fibroblasts for rejuvenating the skin. 6 Regenerative medicine, which uses stem cells and growth factors produced by the body, is an alternative therapeutic strategy for repairing damaged tissues. However, there are still few reports on the anti-aging effects provided by the SVF derived from adipose tissue.
In this way, the present study's objective was to evaluate the effects of SVF in stimulating neocollagenesis and compare its effects with those of a common use synthetic cutaneous filler (calcium hydroxyapatite).
A prospective, comparative controlled study was carried out at the Dermatology Department of the Universidade de Mogi das Cruzes (São Paulo State, Brazil), including 10 female patients (aged between 30 and 45 years, with Fitzpatrick skin phototypes I to V) who had pronounced nasolabial folds.
The patients agreed to participate in the study and signed a consent form. The institution's Research Ethics Committee approved the study.
The exclusion criteria were: pregnancy and breast feeding, immunosuppression history, immune deficiency disorders or use of immunosuppressive drugs, decompensated comorbidities, keloid or hypertrophic scarring history, skin treatment with laser or other devices in the six months prior to the beginning or during the course of the study, and previous use of botulinum toxin, fat injections or filling substances in the area to be treated.
The sample was divided into two groups: Group 1 (5 patients who underwent SVF application bilaterally in the nasolabial folds region), and Group 2 (5 patients who underwent the application of calcium hydroxyapatite synthetic filler in the same region).
Evaluation methods: included clinical examination and photographic analysis before and after treatment, and histological evaluation with staining usually employed in the analysis of tissues (hematoxylin eosin - HE) and staining specifically used for collagen fibers (picrosirius).
Obtaining the adipose tissue: a mini liposuction was performed on the posterior face of the thigh in order to obtain subcutaneous adipose tissue. The procedure was performed in the operating room with appropriate asepsis and antisepsis measures. Approximately 50ml of fat were aspirated by non traumatic manual technique under low pressure.
Obtaining the SVF: a) washing of the material obtained by mini liposuction with PBS solution (phosphate-buffered saline solution) in order to remove debris, and red cells; b) separation into 3 tubes containing 1g of adipose material, and 1 ml of collagenase (Sigma type); c) immersion of the tubes in water at 37º C with constant agitation for 45 minutes; d) centrifuging for 10 minutes followed by separation of the parts with the removal of the matrix, with only the SVF and the adipocyte remaining. 6
Injection: asepsis was carried out with a mild and nonabrasive nonalcoholic agent in the treatment areas. The procedure consisted in the injection of 1ml SVF in the deep dermis with a 26 gauge needle, in the nasolabial fold region of Group 1 patients. Group 2 patients were injected with 1ml of synthetic filler (calcium hydroxyapatite) in the deep dermis, with a similar needle, in the same region.
After appropriate asepsis and local anesthesia with lidocaine with epinephrine pretreatment control biopsy was performed with n. 3 punch, in the right retroauricular region. Next, 1 ml SVF and calcium hydroxyapatite were injected in the retroauricular region, aimed at collecting material for the control biopsy procedures, performed after 30 and 90 days.
Two Group 2 patients (calcium hydroxyapatite) abandoned the study and 3 patients remained until the end of the research. The number of patients in Group 1 remained unchanged.
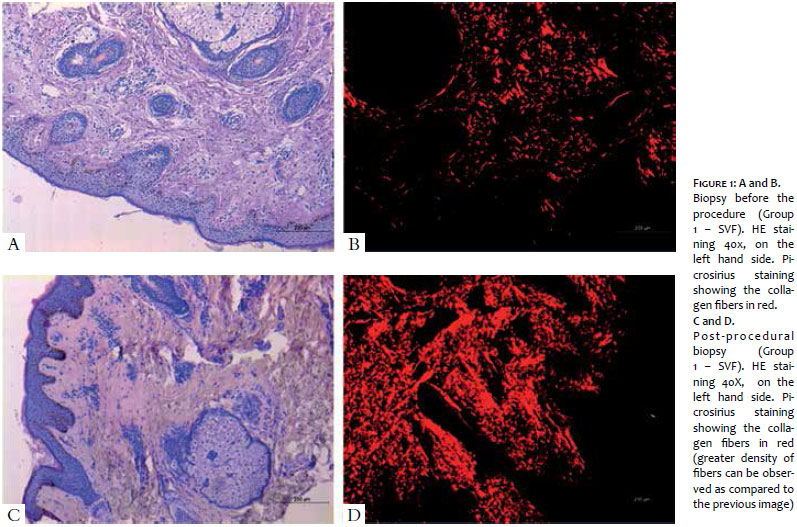
Regarding the histological analysis, evaluations were performed with hematoxylin eosin (HE) and picrosirius, the latter being a specific staining substance for the quantification of collagen in tissues whose collagen fibers are stained in red (Figure 1). The statistical analysis for the quantification of total collagen was initially performed in a generalized manner, without separation of the groups. A baseline mean value of 76% was observed for the collagen in the analyzed tissue, while a value of 84.7% was evidenced after the intervention. Based on the Student t-test, there was absence of statistically significant difference between patients in the pre- and post-treatment experimental timepoints (p = 0.067), nevertheless the results revealed a tendency to statistical significance (probably due to the small number of patients).
Regarding the percentage of collagen, the evaluation of individual groups evidenced values of 78% and 85%, corresponding to the before and after the intervention experimental timepoints, respectively, for Group 1 (SVF). Analogously, those values were 71% and 82.9% in Group 2 (calcium hydroxyapatite) (Graph 1). Based on these data, it was possible to observe that a slightly superior improvement was obtained in Group 1 (SVF). On the other hand, the more encompassing (global) and reliable evaluation led to the conclusion that was absence of statistical significance between the two groups.
The analysis of collagen in the pre-intervention period comparing the two groups using the Mann-Whitney test also showed that there was absence of statistical significance (p = 0.29). This pre-intervention comparative analysis of collagen shows that the comparison was carried out between similar groups without significant individual differences that could lead to a bias in the final results. Based on this same test, the amount of collagen was evaluated in the post-intervention period by comparing Groups 1 and 2, when absence of statistical significance between them (p = 0.54) was evidenced.
As for the dermis' thickness (measured in millimeters - mm), the same analyzes were performed. In the global assessment of patients, the average thickness in the pre-intervention period was 2.22mm, as compared with 1.26mm after the procedure. The Student t test revealed absence of statistically significant difference in the evaluations of the patients' dermis' thickness before and after the procedure (p = 0.21).
In the individual evaluation, Group 1 obtained a pre-procedure average thickness of 2.44mm as compared to 1.72mm in the post-procedure. In Group 2, the pre-procedure average dermal thickness was 1.86mm, as compared to 1.83mm in the post-procedure. The authors obtained reduced thicknesses after the application of the SVF and the filler, outcomes that are not consistent with the increase in the amount of collagen evidenced by the picrosirius staining. One explanation for this discrepancy in the values of the thicknesses would be the fact that the biopsies were not performed by the same examiner physician in the pre and post periods; the histologic evaluation was also not performed by the same professional.
When comparing the pre-intervention dermis' thickness between Groups 1 and 2, it was possible to observe that there was no statistical difference (p = 0.549). The same comparison was carried out after the procedure, also with no observable significant difference between the two groups (p = 0.64).
In the clinical and photographic evaluation, conducted with the assistance of a patient questionnaire and the evaluation of an observer physician, it was possible to observe a moderate improvement, which was classified as a satisfactory final outcome by both observers (Figure 2).
With the advance of aging, the skin undergoes changes such as uneven pigmentation, thinning and loss of elasticity. The factors that trigger the aging of the skin can be intrinsic (or chronological) – which combine into a natural process related to genetic factors, the shortening of telomeres, and the action of free radicals; and extrinsic, corresponding to photoaging – which is the action of solar radiation on the intrinsic factors.
Regenerative medicine, which uses the body's own stem cells and growth factors, is an alternative therapeutic strategy for repairing damaged tissues that is becoming a predominant cell-based therapy. Stem cells derived from adipose tissue (AD-SCs) secrete growth factors such as the vascular endothelial growth factor (VEGF), the insulin-like growth factor (IGF), the hepatocyte growth factor (HGF), and the transforming growth factor beta 1 (TGF-ß1). These proteins control the damage in the neighboring cells. More recently, the production and secretion of growth factors have been identified as an essential AD-SCs' function, and many rejuvenating effects on the skin were demonstrated. 8-10 For example, it was demonstrated that ADSCs stimulated the synthesis of collagen and dermal fibroblast migration during wound healing process. 11 Moreover, the factors secreted in ADSCs protect dermal fibroblasts against oxidative stress induced by UVB radiation and chemicals. 11
Evidence reinforces the critical role of growth factors derived from the ADSCs in wound healing, in the antioxidant effect and in the improvement of the texture and appearance of skin wrinkles, suggesting that they can be good candidates for treating photoaging. 9, 10
The adipose tissue's SVF is a source rich in preadipocytes, mesenchymal stem cells and endothelial progenitor cells, which have great capacity to differentiate into diverse strains. For this reason, it has been widely studied in aesthetical procedures, scars correction and treatment of rhytids and deep furrows in photoaging.
In other recent studies it was also demonstrated that stem cells derived from adipose tissue associated with fat grafts showed satisfactory and longer lasting results, with the survival of the adipocyte being one of the main factors that directly interfere with the success of the grafts.
In the present study, the authors aimed at evaluating the effect of SVF in the treatment of deep furrows and found that there was clinical improvement, perceived by the patients and the observer physician, proven by the increase in the percentage of collagen fibers, which was evidenced by the picrosirius staining. As for the thickness of the dermis, contrary to what was expected, there was no significant increase in the comparison with the control in most patients. One explanation for this may be linked to a technical error related to the biopsy, perhaps performed in areas containing the total thickness of the dermis and subcutaneous tissue, and in areas without the presence of all layers of the dermis, thus justifying the maintenance or even a decrease of the thickness after the procedure. This possible flaw could have been avoided by individually measuring the thicknesses of the upper, medium and deep dermis of the control and in the post-procedure.
Regarding the clinical improvement, when comparing the application of SVF with that of the calcium hydroxyapatite based synthetic filler, it was possible to observe that the latter was slightly greater, which was evidenced in the post-procedure by the effect of the local edema and, in the first months, also proven by the increase in collagen fibers. Regarding the thickness, a technical error bias has probably taken place again, with the expected increase in the dermal thickness not being seen after the use of the filler.
In the evaluation and comparison of the two groups it was not possible to observe superiority of one or the other. The authors note that the percentage results were similar, and there was no statistical significance that could benefit one group or another. It is worth to note that the present study was carried out with a small number of patients and that better analyzes are performed in larger groups, with greater reliability predictors.
In the present study, none of the groups experienced serious complications; only local hematoma (Group 1), and hematoma and edema (Group 2) were observed, with resolution within seven days after the procedure. The patients complained of tolerable pain at the time of application in both groups.
In the present project, it is possible to observe that both techniques for treating facial folds, with the application of SVF or calcium hydroxyapatite based filler, led to satisfactory and similar outcomes, and it was not possible to determine the superiority of one over the other.
The application of SVF is a relatively new technique, which leads to good, histologically confirmed clinical outcomes, however there is need for further study aimed at standardizing the harvesting of the material and developing application techniques.
The use of SVF is a new treatment option for photoaging, according to the observation of the results obtained in the present study. This procedure has been widely discussed and should be improved, especially due to the possibility of being performed with autologous material.
1. Evans MJ, Kaufman MH. Establishment in culture of pluripotential cells from mouse embryos. Nature. 1981;292(5819):154-6.
2. Thomson JA, Itskovitz-Eldor J, Shapiro SS, Waknitz, MA, Swiergiel, JJ, Marshall VS, et al. Embryonic stem cell lines derived from hum an blastocysts. Science. 1998;282(5391):1145-7.
3. Verfaillie CM. Adult stem cells: assessing the case for pluripotency. Trends Cell Biol. 2002;12(11):502-8.
4. Barry FP, Murphy JM. Mesenchymal stem cells: clinical applications and biological characterization. Int J Biochem Cell Biol. 2004;36(4):568-84.
5. Kern S, Eichler H, Stoeve J, Klüter H, Bieback K. Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells. 2006;24(5):1294-301.
6. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R, Mosca JD, et al. Multilineage potential of adult human mesenchymal stem cells. Science.1999; 284(5411):143-7.
7. Jones DL, Wagers AJ. No place like home: anatomy and function of the stem cell niche. Nat Rev Mol Cell Biol. 2008;9(1):11-21.
8. Sharpless NE, DePinho RA. How stem cells age and why this makes us grow old. Nat Rev Mol Cell Biol. 2007;8(9):703-13.
9. Gimble J, Guilak F. Adipose-derived adult stem cells: isolation, characterization, and differentiation potential. Cytotherapy. 2003;5(5):362-9.
10. Prunet-Marcassus B, Cousin B, Caton D, André M, Pénicaud L, Casteilla L. From heterogeneity to plasticity in adipose tissues: site-specific differences. Exp Cell Res 2006;312(6):727-36.
11. Salabian AA, Widgrow AD, Evans GR. Stem Cells in Plastic Surgery: A Review of Current Clinical and Translational Applications. Arch Plast Surg. 2013; 40(6):666-75.
This study was carried out at the Universidade de Mogi das Cruzes (UMC) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}