


Kelly Cristina Signor1; Luciana Gasques de Souza1; Denise Steiner2; Priscilla de Freitas Pereira1; André César Pessanha3; Marco Antônio Soufen4
Pyogenic granuloma or lobular capillary hemangioma is a benign skin and mucous membranes lesion whose etiology is not yet explained. The authors report an atypical and exuberant clinical case of this benign dermatologic condition, clinically simulating malignancy.
Keywords: GRANULOMA, PYOGENIC; SCALP DERMATOSES; HEMANGIOMA, CAPILLARY; MELANOMA
Pyogenic granulomas are benign acquired capillary lesions that affect the skin and mucous membranes and whose pathogenesis is not yet elucidated.1 It is hypothesized to result from mechanical trauma, however the participation of hormonal factors, medicaments, arteriovenous malformations and angiogenic growth factors have also been proposed.2 It has the appearance of an exophytic, friable, fast growing and exulcerated papule or single nodule,1, 3 Due to the fact that some malignant tumors, such as nodular melanomas, mimic pyogenic granulomas, biopsy is necessary for histopathologic analysis in order to prevent delays in the diagnosis and improve the prognosis in case of malignant tumors.
The present report portrays an exuberant and atypical picture of benign dermatologic condition clinically mimicking a malignant lesion.
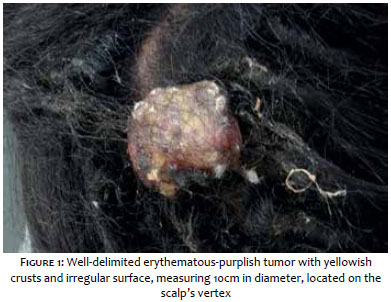
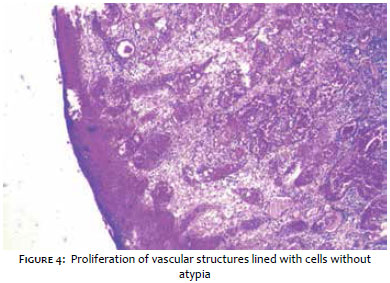
A nineteen year-old female patient sought the dermatology service complaining of the emergence of a lesion in the scalp eight months before, with rapid and progressive growth, accompanied by pain and a yellowish discharge. Dermatological examination showed an erythematous-purplish, well-defined, pedunculated nodule, with exulcerated surface, measuring 10cm in diameter, located on the scalp's vertex (Figure 1). The diagnostic hypotheses were: squamous cell carcinoma, melanoma, Kaposi's sarcoma, cutaneous metastasis, adnexal tumor and pyogenic granuloma. The excisional biopsy of the lesion was carried out (Figure 2), with the histological examination revealing proliferation of vascular structures lined by cells without atypia, suggesting the diagnosis of cutaneous hemangioma of the ulcerated pyogenic granuloma type (Figures 3 and 4). The patient has not had recurrence of the lesion during the two years following its removal.
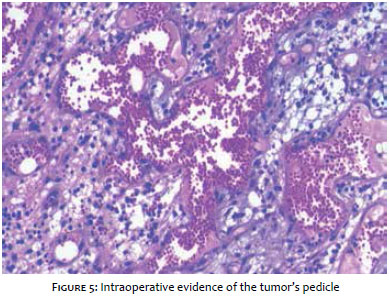
The pyogenic granuloma or capillary lobular hemangioma characterizes a benign vascular proliferation that mainly occurs in body sites exposed to frequent trauma, such as the hands, arms, feet, face, and, less commonly, the trunk and scalp.1,3 It can develop on labial and perianal mucous membranes. It is more prevalent in children and can occur in adults, particularly in pregnant women. Despite its own denomination, pyogenic granuloma is not related to the presence of suppuration, and no specific microorganism can be related to the lesion. In some cases it is associated with secondary infection.4 Its etiology is unknown and is related to a hyperproliferative vascular reaction to a variety of stimuli such as trauma, viral infection, chronic ulcers, female sex hormones and the use of some medications, such as isotretinoin, capecitabine or indinavir.1, 6 Clinically, it presents as a single, nodular or vegetating, friable lesion, varying in color from red to darkened blue. It can be sessile or pedunculated, and develops with rapid growth. It is usually painless, bleeds with minimal trauma and tends to recur.1, 3 Its diagnosis is usually facilitated by history and clinical appearance, nevertheless in some situations it can mimic benign or malignant tumors. The main differential diagnoses are: keratoacanthoma, squamous cell carcinoma, basal cell carcinoma, inflamed seborrheic keratosis, melanocytic nevus, metastatic carcinoma, Kaposi's sarcoma, true hemangioma, vascular tumors of intermediate malignancy and amelanotic or desmoplastic melanoma.4, 5 Due to the fact that some nodular melanomas mimic pyogenic granulomas, biopsy is necessary for pathological studies, thus avoiding delaying the diagnosis. The authors decided to use excisional biopsy in the patient in question, since it was a fast growing exuberant lesion in an atypical location, with suspected malignancy. During the procedure, the visualization of a pedicle in the lesion already suggested the clinical diagnosis of a benign lesion (Figure 5). The histologic examination of the removed specimen evidenced capillary proliferation with radiated pattern and loose edematous collagen matrix in the area near the surface, with the epidermis extending into the lesion's base, leading to the formation of an epidermal collarette and causing, in some cases, the formation of a peduncle. The lobular capillary hemangioma can present mixed inflammatory infiltrate and, in more advanced cases, fibrosis with septa intercepting the lesion can occur, producing a lobular pattern.4-6 Pyogenic granulomas can regress spontaneously; nonetheless most of them require treatment, with the choice of modality depending on the lesion's size and location. The standard therapy is the complete surgical removal and elimination of causative factors. Some authors recommend the use of cryotherapy with carbon dioxide, chemical electrocautery, electrocoagulation and Nd:YAG laser.7, 8 In the present case, a decision was made for performing an excisional biopsy due to the fact that it is a technique that offers low recurrence and rapid clinical resolution.
The present article describes an exuberant, atypical benign and relatively common dermatologic condition, clinically simulating malignancy. It highlights the importance of the detailed dermatologic clinical evaluation and the histological study for diagnostic confirmation.l
1. Piraccini BM, Bellavista S, Misciali C, Tosti A, Berker D, Richert B.Periungual and subungual pyogenic granuloma. Br J Dermatol. 2010;163(5):41-53.
2. Yoradjian A, Azevedo LCM, Cattini L, Basso RA, Zveibil DK, Paschoal FM. Granuloma Piogênico: descrição de dois casos incomuns e revisão da literatura. Surg Cosmet Dermatol. 2013;5(3):2638.
3. Fracoli TS, Bomm L, Sodré SL, Chaves M, Benez M, Silva SCMC. Granuloma piogênico exuberante bilateral: tratamento cirúrgico. Surg Cosmet Dermatol. 2012;4(4):344-7.
4. Zaballos P, Llambrich Á, Cuéllar F, Puig S, Malvehy J. Dermoscopic findings in pyogenic granuloma. Br J Dermatol. 2006;154(6):1108-11.
5. Junck M, Huerter CJ, Sarma DP. Unknown: Rapidly growing hemorrhagic papule on the cheek of a 54-year-old man. Dermatol Online J. 2011;17(1):11.
6. Lee J, Sinno H, Tahiri Y, Gilardino MS. Treatment options for cutaneous pyogenic granulomas: A review. J Plastic Reconstr Aesthet Surg. 2011;64(9):1216-20.
7. Millsop JW, Trinh N, Winterfield L, Berrios R, Hutchens KA, Tung R. Resolution of recalcitrant pyogenic granuloma with laser, corticosteroid, and timolol therapy. Dermatol Online J. 2014;17;20(3).
8. Bourguignon R, Paquet P, Pierard-Franchimont C, Pierard GE. Treatment of pyogenic granulomas with Nd-YAG laser. J Dermatol Treat. 2006;17(4):247-9.
This study was performed at the Universidade de Mogi das Cruzes (UMC) - Mogi das Cruzes (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}