


Thiara Cristina Rocha Lenzi1; Tainah A. Silva2; Eduardo H.K.Oliveira2; Carmélia Matos Santiago Reis3
Having the mastery of surgical techniques, ability to deal with complications and the capacity to train residents in those skills are crucial to the good practice of a dermatologic surgeon. Furthermore, the transmission of clear and objective guidelines to patients has a direct impact on the outcomes of skin surgeries. The present article describes the case of the exeresis of a basal-squamous carcinoma in the scalp with the proposed closure by second intention that developed with infection and necrosis, requiring the team's knowledge and skills to work around the situation. The result of the combination of techniques was satisfactory, showing that proper training is key for a good surgical practice.
Keywords: SKIN NEOPLASMS; RECONSTRUCTIVE SURGICAL PROCEDURES; BLOODLESS MEDICAL AND SURGICAL PROCEDURES; INTERNSHIP AND RESIDENCY
Dermatologic surgeons are key in the dermatological clinical practice. It is crucial that these professionals receive good and solid training in order to enable them to conduct surgical complications that are inherent in the practice of dermatologic surgery. It is also important to highlight that, for the success of a dermatologic surgery, the physician should make sure that the patient has understood all postoperative care prescribed, even the most basic instruction. The purpose of this paper is to describe a case of a simple initial surgical proposal that has developed with complications, demanding that the dermatologic team (surgeon and residents) mastered advanced techniques for the proper management of the condition, obtaining a satisfactory outcome.
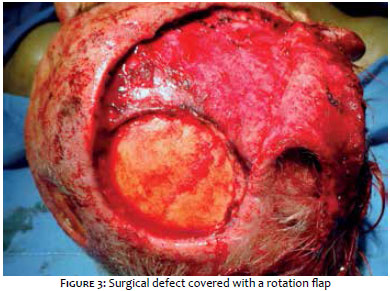
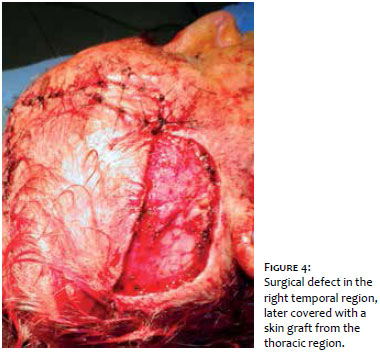
The patient involved is a 76 year-old married man, rural worker, and originary from the Brazilian Mid West State of Goiás. The patient, who did not have comorbidities or was in regular use of medications, was referred to the dermatologic surgery clinic for the treatment of two tumors on the scalp (frontoparietal region) previously histologically diagnosed as basal squamous cell carcinoma and moderately differentiated squamous cell carcinoma, respectively (Figure 1). Due to the facts that the patient was healthy, well informed and accompanied by relatives and that performing a dermatologic surgery with intraoperative control of the margins (Mohs micrographic surgery) was unfeasible, a decision was made for the primary excision of the lesion with safety margins and healing by secondary intention. Systemic antibiotic prophylaxis was prescribed for the postoperative period, with the daily use of occlusive dressing at home, after cleansing the wound with saline solution and applying 1% silver sulfadiazine cream. However, the patient decided to seek support at a basic health center for the daily application of the dressing, where the non-medical professional who provided assistance performed the untimely debridement of the granulation tissue surrounding the wound, which caused necrosis of the underlying periosteum. The patient still developed infection in the surgical wound and impossibility of healing by secondary intention due to loss of tissue. The bone plate of the skull became exposed (Figure 2). Concerned about the appearance of the wound and having pain, the patient returned to the dermatologic surgery service. The authors decided to hospitalize the patient in order to control the local infection with parenteral antibiotic therapy. The care of the surgical wound was then carried out exclusively by a dermatologic surgeon and the department's residents. After the infection was controlled, there was still exposure of the bone plate, which needed to be corrected using a surgical flap/graft technique. A rotation flap was then performed on the bone plate of the parietal-occipital region, combined with a skin graft harvested from the thoracic region and applied to the temporal region of the scalp (Figures 3 and 4). The patient developed with partial loss of the flap and total success of the graft. The region with bone plate exposure could therefore be closed. The patient recovered uneventfully after the combination of surgical techniques, without further complications and with cure of the cancer, attending ambulatory follow up visits to date (Figure 5).
The reconstruction of defects in the scalp, even of small ones, is still a challenge for dermatologic surgeons due to the fact it is an inelastic, convex area and adhered to the galea aponeurotica.1-3 Aimed at achieving good functional and cosmetic outcomes, it is recommended that the simplest possible reconstruction be performed.1, 4 This paper described a case of defects in the scalp after the removal of cutaneous neoplasias, with a simple initial surgical proposal, treated with excision and healing by secondary intention. Nevertheless, it progressed with complications and necrosis of the periosteum due to inadequate treatment of the wound, demanding that the surgeon mastered advanced techniques to properly manage the case. Healing by secondary intention is useful in post-surgical wounds following excision of cutaneous neoplasias for it decreases intraoperative morbidity and the cost of the procedure.5 The granulation tissue is rarely infected, and the pain and bleeding are minimal, while the necessary care to the wound is simple. In addition, the slow healing and repair process itself have protective action against possible recurrences. Furthermore, the absence of grafts or flaps facilitates the early detection of recurrence signs.6 The location of the surgical defect is the defining factor for the healing by secondary intention's cosmetic outcome.7 Complications with this technique are unusual and include exuberant granulation tissue, hypochromic and telangiectasic scars with distortion of the free borders. In the present case, the lack of periosteum after the necrosis compromised the viability of the technique. This paper highlights that the proper training of dermatologic surgeons is crucial for the success of the surgery, as it allows managing and resolving complications that can arise even with the use of simple techniques, such as wound healing by secondary intention. It also shows that the dermatologic surgeons should be able to perform new techniques, such as grafts or flaps, when his or her first choice technique for closing the surgical defect does not prove satisfactory.
The good dermatologist should be able to treat complications through vigorous clinical interventions, as well as to recognize infections and treat them promptly, thus avoiding systemic repercussions. Still, an additional reflection on the doctor/ patient relationship is appropriate: Could it be that the instructions provided in the postoperative period were not sufficiently clear, leading the patient to seek the assistance of a professional from the basic health center? How could the patient have understood that he would be able to apply dressings at home, with only the help of relatives? Should it be stressed that in case of doubt the professional sought should be that who performed the procedure rather than any other? The answers to these questions need to be borne in mind when performing a dermatologic surgery, even those deemed of low complexity, for there is always a potential risk for complications.
1. Desai, SC, Sand JP, Sharon JD, Branham G, Nussenbaum B. Scalp Reconstruction: An Algorithmic Approach and Systematic Review. JAMA Facial Plast Surg. 2015;17(1):56-66.
2. Lee DB, Seong JY, Suh HS, Choi YS. Comet flap for the repair of large surgical defects of the face and scalp. Clin Exp Dermatol. 2015;40(6):708-10.
3. Fowler NM, Futran ND. Achievements in scalp reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2014;22(2):127-30.
4. García del Campo JA, García de Marcos JA, del Castillo Pardo de Vera JL, García de Marcos MJ. Local flap reconstruction of large scalp defects. Med Oral Patol Oral Cir Bucal. 2008;13(10):E666-70.
5. Donaldson MR, Coldiron BM. Scars after second intention healing. Facial Plast Surg. 2012;28(5):497- 503.
6. Bastazini Júnior I, Contin LA, Alves CJM, Nascimento CMSA. Cicatrização por segunda intenção de asa nasal: revisando antigos conceitos. Surg Cosmet Dermatol. 2009;1(4):196-7.
7. Mott KJ, Clark DP, Stelljes LS. Regional variation in wound contraction of mohs surgery defects allowed to heal by second intention. Dermatol Surg. 2003;29(7):712-22.
This study was conducted at the Hospital Regional da Asa Norte, State Health Secretariat, Federal District (HRAN/SES/DF) - Brasília (DF), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}