


Ticiana de Andrade Castelo Branco Diniz1; Maria Isabel Ramos Saraiva2; Marcella Amaral Horta Barbosa3; Larissa Karine Leite Portocarrero4; Thais Amaral Carneiro Cunha5; Neusa Yuriko Sakai Valente6
Tumoral melanosis is a histological term used to refer to a nodular accumulation of melanophages in the dermis, which clinically arises as a pigmented lesion. It is usually associated with the regression of melanomas or of other melanocytic lesions. The authors present the case of a 45-year old man/woman with a pigmented macule on his/her left leg. The lesion was completely excised and diagnosed as a tumoral melanosis.
Keywords: MELANOMA; SKIN NEOPLASMS; DERMATOSCOPY
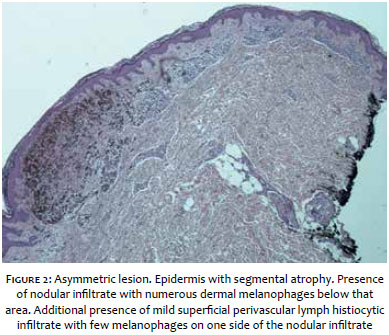
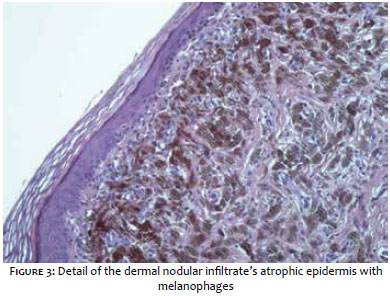
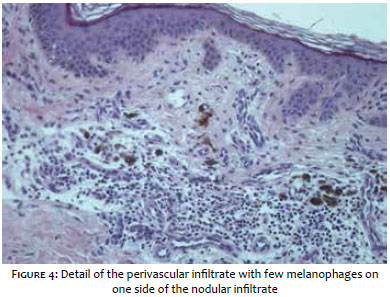
A 45 year-old female patient, with Fitzpatrick's phototype II, sought medical help describing the appearance of a dark spot on the posterior part of the left leg, with spontaneous bleeding, one year before. A blackened lesion with irregular borders and 9mm in its largest diameter was evidenced by the dermatological examination (Figure 1). The dermoscopic examination revealed an asymmetric pigmented lesion, with light brown, dark brown, black and dark blue hues in a homogeneous area, as well as a white-grayish veil (Figure 2). There was absence of vascularization. The patient did not have personal history of skin cancer and family history was negative for melanoma and dysplastic nevus syndrome. Due to the size of the lesion and uneven pigmentation, excisional biopsy was indicated (Figures 3 and 4). Histologic examination revealed a rectified fragment of the epidermis, with nodular infiltrate containing numerous melanophages in the dermis.
There were melanocytes in the epidermis or dermis - even in semi-serial sections - leading to the diagnosis of tumor melanosis. The examination of the entire cutaneous surface, mucous membranes and accessible lymph nodes was carried out, with absence of any evidence of melanoma. The patient was referred for evaluation of the retina and oncologic staging.
Nodular or tumor melanosis - also known as melanophagocytosis or melanophagic dermatitis - is a term used to denote the histological accumulation of melanophages in the dermis, clinically arising as a pigmented lesion with suspicion of melanoma.1, 2
It is considered a rare condition and there is absence of reports in the literature of cases in children or adolescents.3 Its importance is linked to the association with melanoma regression or satellite metastases.1, 2
Smith and Stehlin described the regression phenomenon in the literature in 1965. It consists in the reduction of a tumor's volume due to the host's immune response, a frequent finding in melanomas.4, 5 Partial regression was observed in about 10% to 35% of primary melanomas, however the full phenomenon is considerably rare. 6, 7
Tumor melanosis is considered a rare variant of the totally regressed melanoma.8, 9 Its histology seems to correspond to that of residues of pre-existing malignant melanomas (MM).10 Nevertheless, there are reports of cases of non-melanoma melanocytic lesions.2
In this manner, the nature of the underlying lesion cannot be determined until some melanoma residue is identified. Epithelial neoplasms, such as pigmented basal cell carcinoma and dysplastic nevi, Clark's nevus, Bowen's disease, fungoid mycosis and solar lentigo, are diagnoses that can be found following careful analysis.8, 9
Histological findings suggestive of tumor melanosis after MM regression consist of hyperplasia of the epidermis, presence of melanophages in the dermis, focal fibroplasia, fibroplasmocytic infiltrate and regression findings. Sometimes the diagnosis is confirmed by residual MM findings.6 In case of doubt, the histogenesis of melanized cells, the immunohistochemistry, the positivity for CD68 and negativity for S-100, HMB-45 and Melan-A confirm the histiocytic nature of the lesions. 9
Despite the fact that the careful sequential analysis of the cuts has not shown any sign of MM in the case studied, possibility of a completely regressed MM could not be excluded.
Unlike MMs, tumor melanosis cannot be treated, with absence of well-established prognosis or follow up in the literature - nonetheless attention should be devoted to the possibility of melanoma with total regression. There are cases of metastatic MMs arising after the diagnosis of tumor melanosis.2, 9 Due to the uncertainty about the exact nature of the previous lesion (in situ melanoma, superficial melanoma or non-melanoma melanocytic lesions), the prognosis becomes impossible,8, 9 resulting in the fact that therapeutic recommendations remain undefined to date.9 The complete excision of the lesion with appropriate margins seems to be the appropriate approach. A powerful source of additional data can be the sentinel lymph node mapping.8 It is suggested that a similar follow-up be implemented due to the high risk of melanoma,9 however this possibility should be discussed with the patient. Due to the rarity of the condition and uncertainty of the prognosis, additional studies aiming at better monitoring these patients are necessary.
1. Dogruk Kacar S, Ozuguz P, Karaca S, Aktepe F. Tumoral melanosis in an adolescente after trauma: a clinicopathological dilemma. Pediatr Dermatol. 2014;31(2):e69-70.
2. Flax SH, Skelton HG, Smith KJ, Lupton GP. Nodular melanosis due to epithelial neoplasms: a finding not restricted to regressed melanomas. Am J Dermatopathol. 1998; 20(2):118-22.
3. Ng H, Chave TA. Tumoralmelanosis as a manifestation of a completely regressed primary melanoma with metastasis. Br J Dermatol. 2006; 155(3):627-8.
4. Smith Jr JL, Stehlin Jr. L. Spontaneous regression of primary malignant melanoma with regional metástases. Cancer. 1965;18:1399-415.
5. Blessing, K; Mclaren, K. M. Histological regression in primary cutaneous melanomas: recognition, prevalence and significance. Histopathology. 1992;20(4):315-22.
6. Barnhill RL, editor. Malignant Melanoma. In: Pathology of melanocytic nevi and malignant melanoma, 2nd ed. New York: Springer, 2004. p. 342.
7. Menzies SW, McCarthy WH. Complete regression of primary cutaneous malignant melanoma. ArchSurg 1997; 132(5):553-6.
8. Satzger I1, Völker B, Kapp A, GutzmerR. Tumoral melanosis involving the sentinel lymph nodes: a case report. J Cutan Pathol. 2007;34(3):284-6.
9. LeBoit PE1. Melanosis and its meanings. Am J Dermatopathol. 2002;24(4):369-72.
10. Massi G. LeBoit PE. Regressing and regresses melanoma. In: Massi G. Le- Boit PE, eds. Histological diagnosis of nevi melanoma. Darmstadt: Springer; 2004. p. 625.
This study was performed at the Hospital do Servidor Público Estadual do Estado de São Paulo - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}