


João Marcos Góes de Paiva1; Marta Regina Machado Mascarenhas1; Laís de Abreu Mutti1; Ival Peres Rosa1; Mauro Yoshiaji Enokihara2
The lips are a preferred site for carcinomas. Roughly 95% of tumors in the lips involve the lower lip, with 90% being squamous cell carcinomas. Surgery is the treatment of choice and has a good prognosis when diagnosis is performed early. Defects involving less than half of the lower lip can be closed using the edge-to-edge technique, whereas larger defects require greater technical complexity of methods and have increased risk of complications. The present article describes a straightforward technique for reconstructing these defects, using edge-to-edge suture, without necessity ofV or W shaped excisions, and with good aesthetic and functional outcomes.
Keywords: CARCINOMA, SQUAMOUS CELL; LIP NEOPLASMS; RECONSTRUCTIVE SURGICAL PROCEDURES
Nonmelanoma skin cancer is the most common tumor in Caucasians. Its preferred locations are the head and neck.1 Lips are often affected, with 95% of tumors in this region being located in the lower lip. In most cases, these are squamous cell carcinomas (SCCs).2
The lower lip SCC corresponds to a percentage ranging from 25% to 30% of all oral cancers. It affects more men over 50 years of age, who have had significant exposure to the sun throughout their lives. Risk factors such as smoking habits, drinking alcohol and immunosuppression following kidney transplantation can be associated with this neoplasm.3
Despite the good prognosis when diagnosed at an early stage, the occurrence of lymph node metastases can reach 20% of cases.3
The treatment of choice for these tumors of the lower lip is surgery with a safety margin. Mohs surgery has been used with increasing frequency and good results, however it is not widely available in the Brazilian medical care services, being expensive and of complex implementation, therefore inaccessible to most patients. The excisional surgery in such cases should be carried out with a 7mm to 10 mm safety margin, which leads to recurrence rates and clinical outcomes similar to those of the Mohs surgery,3 in addition to having a shorter execution time, being cost effective and technically simpler.
Lesions involving up to half of the lower lip can be primarily sutured.4 Smaller lesions can be excised in a "V" shape, while larger lesions are excised using the "W", in order to avoid trespassing the mental sulcus.4
Defects larger than half of the lower lip generally cannot be primarily closed without increasing the tension at the edges of the wound and causing the occurrence of microstomy. As a result, it is necessary to carry out flaps with tissue originally from the upper lip and perioral regions.5
The likelihood of having to implement this type of flap often inhibits dermatologic surgeons, who choose not to perform surgeries on the lower lip due to the great technical difficulty, the long surgical time and the high risk of complications. The technique described in the present paper is fast and easy to perform, with good outcomes and low risk of complications.
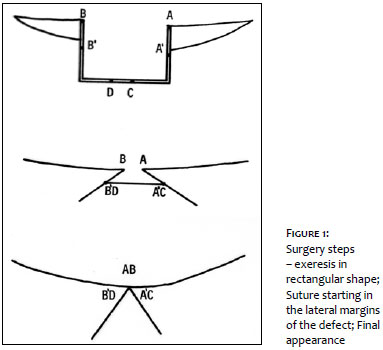
It consists in the resection of the tumor with a 5mm to 8 mm safety margin and total tissue thickness (including the oral mucosa), so as to obtain a rectangular defect. The suture is initially carried out in the lateral edges, bringing THE POINTS B'AND D / A'AND C TOGETHER, AS WELL AS THE BORDERS of the vermilion, FINISHING with the suture of the vermilion (Figure 1).
Figure 2 depicts the initial marking of rectangular shape and the final aspect of the surgery. Figure 3 shows the late postoperative period in the same patient, with good aesthetic result. The surgery, like any edge-to-edge reconstruction of the lower lip, causes a discreet initial microstomy, which improves after a few months of development.
The lower lip SCC is a common tumor in the dermatological sphere. The treatment of choice is surgical, with good prognosis when performed early. Nevertheless, there is a significant risk of cervical metastases, and the search for affected lymph nodes is included in the initial clinical evaluation of these patients.
The choice of the technique to be used in the reconstruction of the lower lip should consider the functional and aesthetic aspects of the lips, in addition to the size of the defect. Defects smaller than half of the lower lip can be corrected with edge-to-edge suture. It is important to note that this type of reconstruction always leads to some degree of microstomy. Although there are a number of techniques for the reconstruction of defects greater than half of the lower lip, most of them involve complex surgeries, often difficult to implement for the dermatologic surgeon. The authors have described a simple technique that can be performed by dermatologic surgeons under local anesthesia and leads to good aesthetic and functional results.
1. Kayabasoglu G, Nacar A, Baker SR. A Novel Flap Technique for Repairing Large Lower Lip Defects. Aesthetic Plast Surg. 2015;39(2):231-4.
2. Wollina U. Reconstructive surgery in advanced perioral non-melanoma skin cancer. Results in elderly patients. J Dermatol Case Rep. 2014 Dec 31;8(4):103-7.
3. Hasson O. Squamous cell carcinoma of the lower lip. J Oral Maxillofac Surg. 2008;66(6):1259-62.
4. Campbell JP. Surgical management of lip carcinoma. J Oral Maxillofac Surg. 1998;56(8):955-61.
5. Cupp CL, Larrabee WF. Reconstruction of the Lips. Otolaryngol Head Neck Surg. 1993;(4):46-53.
Trabalho realizado no Departamento de Dermatologia da Universidade Federal de São Paulo (Unifesp) - São Paulo (SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}