


Gabriela Horn1; Mariana de Jesus Oliva Siebel2; Yana Lya de Almeida Leda1; Daniela Sanchez Facci1; Diego Leonardo Bet3
The acquired perforating dermatosis is constituted by a group of diseases whose main characteristic is the transepithelial elimination of altered dermal material. It has the clinical appearance of crateriform papules or nodules, with central keratotic plug, which may suggest some kind of transepithelial purging; nevertheless the final diagnosis is histologic. The dermoscopic examination is a useful tool that helps to exclude similar dermatoses, such as nodular prurigo and hypertrophic lichen planus. The present article discusses the clinical and dermoscopic correlation of this dermatosis.
Keywords: DERMOSCOPY; PRURIGO; DIAGNOSIS, DIFFERENTIAL
Acquired perforating dermatosis (APD) constitutes a group of dermatoses that are characterized by transepithelial elimination of altered dermal material (collagen, elastic fibers and/or hair follicle).1-3 It occurs in adulthood and is commonly associated with diabetes mellitus and chronic kidney disease (up to 10% of patients undergoing dialysis). It is also found in association with liver failure, hypothyroidism, hyperparathyroidism, pulmonary fibrosis, HIV/AIDS, scabies and malign neoplasias.4
From the clinical point of view, there is emergence of papules or crateriform nodules with a central keratotic plug that may have follicular pattern. The most affected body sites are the extensor surface of the limbs and the trunk. Itching is common, with frequent excoriations and crusting. New lesions can arise through the Koebner phenomenon.2
In light of histologic findings, APD can be classified into: reactive perforating collagenosis, serpiginous perforating elastosis, perforating folliculitis and Kyrle's disease. There can be superposition of more than one type in the same patient, the coexistence being more common in dialysis patients. In this way, it is recommended that more than one biopsy be carried out.1
There is no established standard treatment; the most frequently mentioned in the literature are: topical/intralesional corticosteroid, retinoid, allopurinol and phototherapy. Where there is an underlying disease, its control can lead to the improvement of APD. Pruritus can be controlled with anti-histamines.
In this paper, the authors describe two cases of APD, correlating clinical and dermoscopic aspects.
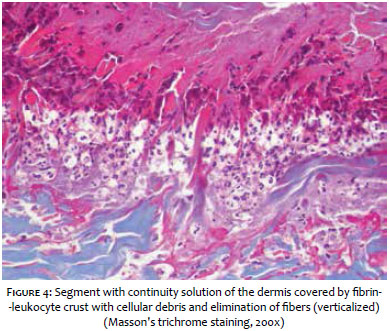
Case 1: A 63 year-old male patient experienced the abrupt onset of intensely pruritic lesions on the dorsum, which quickly progressed to the cervical region and proximal members in two weeks. The dermatological examination revealed: multiple umbilicated papules and nodules, of brownish color and varying sizes, some of follicular pattern, with central keratotic plug (Figure 1). Comorbidities: hypertension, diabetes mellitus, ischemic heart disease, peripheral vascular disease and chronic renal insufficiency/dialysis. The dermoscopic examination with polarized light allowed observing a peripheral brown-grayish amorphous area with a white keratotic center, with depressed appearance and presence of a yellowish area (Figures 2 and 3). The histology of the specimen (obtained through a fusiform excision on the dorsum) showed continuity in the papillary dermis, covered by a thick necrotic crust containing cellular debris, neutrophils, verticalized collagen fibers with transepithelial elimination, characterizing a reactive perforating collagenosis (RPC) (Figure 4). The patient was treated with 0.05% betamethasone dipropionate and topical 3% salicylic acid, in addition to 15mg/day mirtazapine for controlling the pruritus. It showed improvement in 30 days.
Case 2: A 46 year-old male patient reported the appearance of pruritic lesions in the upper limbs six months before. The dermatological examination revealed multiple brownish papules with central keratotic plug (Figure 5). Background: hypertension, diabetes, chronic renal failure requiring dialysis. Dermoscopy with polarized light revealed a peripheral erythematous-grayish amorphous area, with white keratotic center, depressed appearance and a small yellow-brownish area. The histology showed similar findings to those of the previous case. The patient was treated with betamethasone valerate twice a day, with improvement of the picture and the absence of new lesions.
Reactive perforating collagenosis is characterized by the transepidermal elimination of collagen. It can be primary (a possible autosomal recessive inheritance) or secondary (acquired), associated with systemic diseases.3 The clinical and epidemiological findings in the present report were consistent with the literature (adult diabetic and renal patient, requiring dialysis, with multiple keratotic, umbilicated, pruritic papules prevalent in the trunk).
The pathogenesis is not known and alterations in fibroelastic bundles can be partly explained by the diabetes. In addition, trauma would be another contributing factor, as the Koebner phenomenon is observed in sites with injuries, insect bites, herpes zoster and acne scars.3
The final diagnosis was confirmed by the histology, with the observation of a cupuliform depression filled with degenerated basophilic material, and the presence of foci of ulceration and vertically oriented collagen fibers crossing the dermal-epidermal junction that are better visualized using the Masson's trichrome staining (it stains the collagen in blue). In addition to the biopsy, performing dermoscopy is a useful tool, helping to exclude similar dermatoses, such as nodular prurigo and hypertrophic lichen planus. According to Errichete et al., the white starburst pattern (white lines arranged radially) on erythematous-brownish background is seen in nodular prurigo, while there is presence of whitish crossed lines (Wickham striae) in hypertrophic lichen planus.5 In the authors' dermoscopic analysis, it was possible to observe a central white area, yellow plugs of keratin with variable size (possibly corresponding to the area of fibrosis and extrusion of dermal material), a keratotic collarette with a brown-grayish amorphous or erythematous area surrounding it, possibly due to inflammatory reaction. The absence of other described patterns helped the authors to exclude those dermatoses.
With the two cases described in the present paper, the authors highlight the peculiar clinical presentation of perforating dermatosis and the importance of dermoscopy as an auxiliary method in the diagnosis.
1. Ramirez-Fort MK, Khan F, Rosendahl CO, Mercer SE, Shim-Chang H, Levitt JO. Acquired perforating dermatosis: a clinical and dermatoscopic correlation. Dermatol Online J. 2013;19(7):18958.
2. Akoglu G, Emre S, Sungu N, Kurtoglu G, Metin A. Clinicopathological features of 25 patients with acquired perforating dermatosis. Eur J Dermatol EJD. 2013;23(6):864-71.
3. Castro LGM, Nogueira MF, Valente NYS. Colagenose reativa perfurante adquirida associada a insuficiência cardíaca congestiva. Bras Dermatol. 2001;76(4):437-9.
4. Tilz H, Becker JC, Legat F, Schettini APM, Inzinger M, Massone C, et al. Allopurinol in the treatment of acquired reactive perforating collagenosis*. An Bras Dermatol. 2013;88(1):94-7.
5. Errichetti E, Piccirillo A, Stinco G. Dermoscopy of prurigo nodularis. J Dermatol. 2015;42(6):632-4.
This study was performed at the Hospital do Servidor Público Municipal de São Paulo (HSPM-SP), SP, Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}