


Emerson de Andrade Lima
Introduction: Despite the existence of well-established therapeutic approaches, static glabellar wrinkles arise as a challenge. The subincision is a technique commonly used for the improvement of these lesions.
Objectives: The present article proposes a new methodology for the undermining of static glabellar wrinkles termed and registered by the author as Dermal Tunneling (TD®).
Methods: Twelve patients who underwent dermal tunneling carried out by the same physician, according to the same methodology, were retrospectively assessed through direct observation, photographic analysis and self-assessment questionnaires.
Results: All patients reported that the results were good or very good. The evaluation carried out by two independent dermatologists, based on before and after photographs, showed that two patients had regular outcomes (25% improvement), five had good outcomes (50% improvement) and five had very good outcomes (75% improvement).
Conclusion: Dermal Tunneling (TD®) can be considered an effective, safe and reproducible treatment.
Keywords: WRINKLE; SKIN; THERAPEUTICS
The presence of wrinkles on the forehead and glabella - even in the absence of contraction of the corresponding muscles - gives rise to static lines, which are usually difficult to be soothed.1 The use of botulinum toxin leads to good results in dynamic wrinkles, nevertheless the response is unsatisfactory regarding deep static wrinkles, entailing that the treatment is commonly supplemented with cutaneous fillers.1, 2 Subcutaneous incision has also been proposed for the treatment of these rhytids, which are usually comparable to scars due to their depth, rigidity and inflexibility. Initially described by Orentreich and Orentreich,3 this technique is based on the rupture of fibrotic bundles and the triggering of inflammatory response, including bleeding, which culminates in the production of collagen.3, 4 Needles with specific characteristics have been used by different authors to perform this technique, among them the 19G, 20G, 21G, 18G1, 5 Nokor, with particular technical advantages.4-6 Adverse effects such as edema, hematoma and pain can be evidenced in the immediate post-procedure period. Among possible late complications are post-inflammatory hyperpigmentation, overcorrection of the treated depression and fibrotic nodules.4 These complications can be prevented or adequately managed when an experienced and discerning professional performs the intervention.7 The present paper proposes the correction of glabellar static wrinkles using a new device and an easily implementable methodology called Dermal Tunneling (TD® - from the Portuguese Tunelização Dérmica).
Medical records of 12 patients who attended the author's private practice and the Cosmiatry Clinic of the hospital Santa Casa de Misericórdia do Recife (PE, Brazil) were retrospectively evaluated from January 2013 to January 2015. All patients had static glabellar wrinkles and were treated with TD®, having undergone the same procedure, which was performed by the same doctor. All patients had never received any kind of treatment in the glabellar area before. Photographic records were performed by the same researcher, using the same digital camera and under the same lighting conditions, immediately before and two months after a single intervention. The assessment of the results was performed through the analytical photographic comparisons carried out by two independent dermatologist physicians according to the following scale: moderate (25% improvement), good (50% improvement), very good (75% improvement) and excellent (100% improvement). A self-assessment questionnaire was applied to the patients aimed at evaluating their satisfaction with the procedure's outcome, according to the following ratings: bad, good, very good and excellent.
The study complied with the guidelines recommended by the Declaration of Helsinki.
Description of the surgical technique
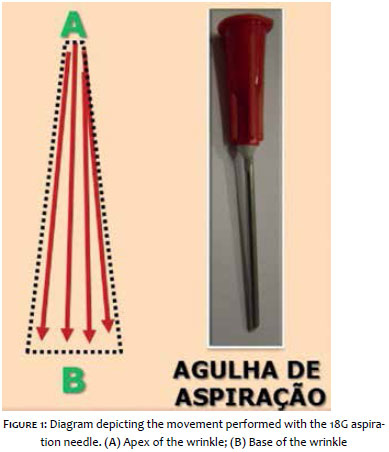
The device used to perform the TD® is a sterile aspiration needle, 1.20 x 25mm 18G x 1". The treatment should be performed in a procedure room carefully prepared for surgery. Fist of all, the area to be treated was marked, with lines having been drawn on the static wrinkles to be corrected. Next, antisepsis with 2% chlorhexidine was carried out and infiltrative anesthesia with 2% lidocaine (without vasoconstrictor) was performed. The aspiration needle was then introduced transepidermally up until the depth of the dermis, at the most distal point of the wrinkle (point A). Then was moved toward the base of the wrinkle (point B), producing a path in the shape of a tunnel. In order to achieve that, the needle was moved back and forth, with every movement performed between A and B progressively creating a tunnel. It is proposed that three or four tunnels be produced using the same procedure - introducing the needle in same initial orifice (point A) and moving it toward the base of the wrinkle (point B). This process results in the creation of three or four vertical hematic columns arranged in parallel, causing the detachment of the bundles and in the hematic filling of the wrinkle (Figure 1). After the procedure, the patients received micropored dressing (which was removed on the following day) and were instructed to use only industrialized SPF 60 sunscreen.
In the self-assessment questionnaires, all 12 patients (7 women, 5 men) rated the outcomes as good or very good. Based on before-and-after photographs, the assessment carried out by two independent dermatologist physicians revealed a similar perception of the degree of improvement: two patients had 25% improvement (moderate), five had 50% improvement (good), and five had 75% improvement (very good). The pain during treatment was considered tolerable. The patients studied were aged between 42 to 60 years, and had Fitzpatrick phototypes (1975) ranging from II to IV. The return to professional activities took place between the fifth and seventh day after the procedure, with significant reduction of the edema and hematoma. There was absence of complications, such as infection, overcorrection, postinflammatory hyperpigmentation, or persistent fibrotic nodules (Figure 2). Among the patients evaluated, five have already been followed up for 24 months, with permanence of the satisfactory outcomes.
Despite the great number of proposals put forward, the treatment of glabellar wrinkles is still a challenge with difficult solution.2 They are a frequent complaint in dermatologic practices and are often only partially corrected with the application of botulinum toxin, for even when attenuated, they continue to cause annoyance due to their static wrinkle condition.8 The filling of this almost cicatricial depression with hyaluronic acid offers dubious safety, due to the risk of intravascular injection and variable results.2, 8
The author proposes a new surgical approach to these lesions, based on an attempt to optimize the results observed with the already existing undermining techniques,3, 5 standardizing the intervention methodology and the specific tools, and which can be reproduced by other physicians in many patients.
The dermal tunneling (TD®) technique, following the methodology described above, was effective in treating static glabellar wrinkles.
The outcomes were promising and consistent with the expectations of the author and patients, giving rise to the suggestion of inclusion of the proposed methodology in the therapeutic armamentarium to treat these lesions.
Pain and discomfort reported by the patients in the intra- and postoperative were in line with the expected.
The absence of complications in the postoperative encourages the treatment of other patients.
The author suggests the assessment of the technique in other groups aiming at confirming the results and conclusions presented in this paper.
1. Almeida ART, Marques ERMC, Kadunc BV. Rugas glabelares: estudo piloto dos padrões de contração. Sug Cosmet Dermatol. 2010; 2(1):23-8.
2. Dubina M, Tung R, Bolotin D, Mahoney AM, Tayebi B, Sato M, et al. Treatment of forehead/glabellar rhytide complex with combination of botulinum toxin and hyaluronic acid versus botulinum toxin a injection alone: a split face, rather-blinded, randomized control trial. J Cosm Dermatol. 2013 ;12(4):261-6.
3. Orentreich DS, Orentreich N. Subcutaneuos incisionless (subcision) surgery for correction of depressed scars and wrinkles. Dermatol Surg; 1995;21(6):543-9.
4. Hexsel DM, Mazzuco R. Subcision: uma alternativa cirúrgica para a lipodistrofia ginóide (celulite) e outras alterações no relevo corporal. An Bras Dermatol. 1997: 72(1) :27-32.
5. AlGhamdi KM. A better way to hold a Nokor needle during subcision. Dermatol Surg. 2008;34(3):378-9.
6. Balighi K, Robati RM, Moslehi H, Robati AM. Subcision in acne scar with. and without subdermal implant: a clinical trial . J Eur Acad Dermatol Venereol. 2008, 22(6):707-11.
7. Hexsel DM, Mazzuco R. Subcision: a treatment for celulite. Int J Dermatol. Int J Dermatol. 2000;39(7):539-44.
8. Kim HS, Kim C, Cho H. A study on glabellar wrinkle patterns in Koreans. J Eur Acad Dermatol Venereol. 2014; 28(10): 1332-9.
This study was performed at the Santa Casa de Misericórdia do Recife (PE), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}