


Sadamitsu Nakandakari1; Ana Paula Cota Pinto Coelho2; Gabriela Franco Marques3; Cleverson Teixeira Soares4
Melanonychia corresponds to color patterns in the nail plate, ranging from brown to black. It is a diagnostic challenge due to the fact it has several differential diagnoses, including benign and malignant entities. There are no reports of pigmented fibroma of the nail matrix causing striata (or longitudinal) melanonychia. In light of this fact, the authors report a case of melanonychia striata secondary to pigmented fibroma of the nail, with clinical examination and dermoscopic findings suggestive of nodular melanoma.
Keywords: NAILS; MALFORMED NAILS; NEOPLASMS; FIBROMA
Melanonychia is the color, ranging from brown to black, of the hands' or feet' nail plates. It may be secondary to exogenous pigments including tobacco, dirt and tar; fungal infections; bacterial infections such as Pseudomonas aeruginosa and Proteus spp; and subungual hematoma caused by trauma. Clinical findings are variable according to the etiology. Anamnesis, dermoscopy of the nail plate, direct mycological examination and culture for fungi and bacteria are crucial for the diagnosis. 1, 2
The production of melanin in the nail matrix - in most cases in the form of a longitudinal band - also manifests clinically as melanonychia, and can be called longitudinal melanonychia or melanonychia striata. It occurs in benign diseases, such as nevi and lentigines of the nail matrix, and in various inflammatory, traumatic and iatrogenic disorders responsible for the activation of the matrix's melanocytes (hypermelanosis). Melanonychia striata can still be secondary to melanoma, and its diagnosis remains a challenge for dermatologists. 1, 3
Ungual fibroma is a benign tumor of the connective tissue that arises as an asymptomatic, skin color nodule. It usually originates in the proximal border of the nail, with rare cases arising in the matrix region. Trauma is the most important factor associated with the lesion's etiology.4, 5 There are no reports in the international literature of pigmented ungual matrix fibroma causing longitudinal melanonychia. In light of this fact, the authors of the present study describe a unique case of melanonychia striata secondary to a fibroma associated with epithelial hyperpigmentation, with clinical and dermoscopic findings suggestive of nodular melanoma.
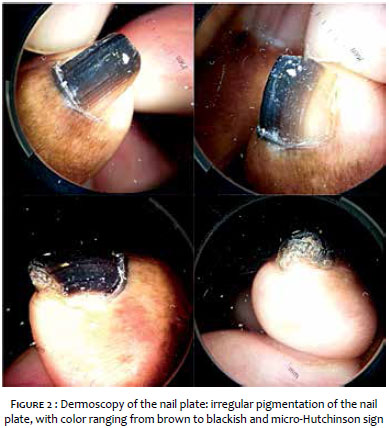
A 68 year-old, dark skinned female patient complained of the darkening of the nails of the feet and hands, that had taken place more than ten years before. Examination revealed the presence of melanonychia striata in several nails of the toes and fingers, compatible with racial melanonychia. However, the hyperpigmentation of the fourth toe of the right foot was more exuberant, with involvement of 75% of the nail plate. In addition, it had ungual hyperkeratosis and transverse hypercurvature of the nail (Figure 1). Dermoscopy allowed visualizing uneven pigmentation in the nail plate, with color ranging from brown to black, besides micro-Hutchinson sign (Figure 2).
The nail plate was avulsed, evidencing a papular pigmented lesion in the nail matrix region. Intraoperative dermoscopy revealed a blackened lesion with gray areas simulating blue-whitish veil and microinvasion signs in the proximal ungual fold. In light of these findings, the hypothesis of nodular melanoma was formulated and an excisional biopsy was carried out (Figures 3 and 4).
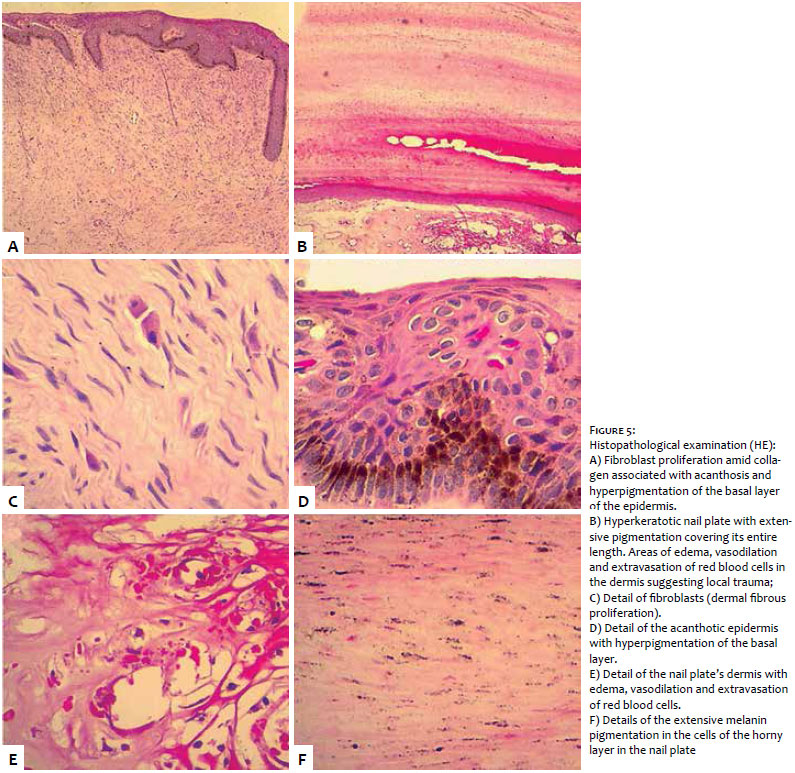
The pathological examination evidenced a fibrous proliferation in the dermis with hyperpigmentation of the basal layer, compatible with pigmented fibroma, leading to the exclusion of the hypothesis of melanocytic origin for the lesion (Figure 5).
Melanonychia can have various etiologies, from physiological causes to malign neoplasia - hence the importance of the early etiologic diagnosis. In this context, dermoscopy of the nail plate is highlighted as a useful test for differentiating benign and malignant lesions. 6
According to the Consensus on nail plate dermoscopy in melanonychia, a brown background associated with parallel lines of regular spacing and width, in the same color, suggests the presence of a benign lesion (nevus or lentigo), while a brown background associated with longitudinal lines irregular in color, width, spacing, and parallelism suggests the existence of melanoma. Nonetheless, the decision to excise the lesion should be based on the clinical criteria rather than on the patterns observed in the dermoscopy of the nail plate. 7, 8
In the present case, the patient had melanonychia in several toenails, characterized by longitudinal homogeneous parallel lines, gray in color and regular in their spacing, thickness and color, characterizing a typical presentation of racial melanonychia. However, the nail plate of the fourth toes of the right feet stood out once it had longitudinal lines with irregular spacing and thickness, and color ranging from brown to black and a blue-grayish area in its central portion, which are findings suggestive of melanoma. Corroborating with this hypothesis, the pigmentation extended over the proximal nail fold (micro-Hutchinson sign).
These facts led the authors to decide for avulsing the nail plate and performing an excisional biopsy. During the surgery, dermoscopy of the blackened lesion evidenced in the nail matrix region revealed multiple colors with irregular longitudinal lines, favoring the initial hypothesis of nodular melanoma. The lesion was then complete excised with 1mm deep shaving.
The material was sent for histological examination, which evidenced fibrous proliferation of the dermis, consisting of spindle-shaped fibroblasts amid dense collagen fibers and acanthotic epidermis with hyperpigmentation in the basal layer, without melanocytic proliferation. The nail plate showed epidermis with hyperkeratosis and melanin hyperpigmentation, and underlying dermis with edema and vascular proliferation. These findings ruled out the melanocytic origin of the lesion, while being consistent with the diagnosis of pigmented fibroma. The presence of edema, vasodilation and extravasation of red blood cells in the dermis suggests local trauma, the main etiological factor for the development of ungual fibromas.
Ungual fibromas are uncommon benign tumors of the fibrous tissue. Solitary lesions are denominated acquired nail fibrokeratomas while multiple lesions are associated with tuberous sclerosis,in this circumstance being called Koenen tumors. There is no histological difference between the two variants. The lesions are usually asymptomatic and arise as pinkish or skin color nodules with globoid morphology. They are most often located periungually, but rarely are subungual, originating from the nail matrix. The treatment is surgical, with the complete removal of the lesion. 5, 9
The fibroma of the nail matrix cases described in the literature manifested with thinning of the nail plate, transverse hypercurvature or exophytic growth of the proximal nail border. However, the authors have not found in the literature cases of fibroblast proliferation in nail matrix with characteristics similar to those of fibroma associated with epithelial hyperpigmentation, resulting in melanonychia striata - hence the relevance of the present report. In addition, the clinical examination and dermoscopy findings led to the hypothesis of nodular melanoma, which can only be discarded after histological analysis. The authors emphasize the need for examining the dermoscopic characteristics of the nail plate and of the lesion itself, after avulsion of the nail plate in light of to all cases of melanonychia, although the definitive diagnosis is established only by pathological examination.
1. Di Chiacchio N1, Ruben BS, Loureiro WR. Longitudinal melanonychias. Clin Dermatol. 2013;31(5):594-601.
2. Lam C, Weyant GW, Billingsley EM. Longitudinal melanonychia of the toenail. JAMA Dermatol. 2014;150(4):449-50.
3. Haneke E1, Baran R. Longitudinal melanonychia. Dermatol Surg. 2001;27(6):580-4.
4. Baran R1, Perrin C, Baudet J, Requena L. Clinical and histological patterns of dermatofibromas of the nail apparatus. Clin Exp Dermatol. 1994;19(1):31-5.
5. Cahn RL. Acquired periungual fibrokeratoma. A rare benign tumor previously described as the garlic-clove fibroma. Arch Dermatol. 1977;113(11):1564-8.
6. Bilemjian APJ, Piñeiro-Maceira J, Barcaui CB, Pereira FB. Melanoníquia: importância da avaliação dermatoscópica e da observação da matriz / leito ungueal. An. Bras. Dermatol. 2009;84(2):185-9.
7. Di Chiacchio ND, Farias DC, Piraccini BM, Hirata SH, Richert B, Zaiac M, et al. Consensus on melanonychia nail plate dermoscopy. An Bras Dermatol. 2013;88(2):309-13.
8. Koga H1, Saida T, Uhara H. Key point in dermoscopic differentiation between early nail apparatus melanoma and benign longitudinal melanonychia. J Dermatol. 2011;38(1):45-52.
9. Richert B1, Lecerf P, Caucanas M, André J. Nail tumors. Clin Dermatol. 2013;31(5):602-17.
The present study was conducted at the Instituto Lauro de Souza Lima (ILSL) -Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}