


Sandra Tagliolatto
Radiofrequency is considered a safe and non-invasive method for treating cutaneous sagging and for improvement of the body and facial contours. It has proven effectiveness, which is however limited in the more serious cases of ptosis. The effects of radiofrequency are based on the volumetric heating of the deep dermis, heating the collagen and elastic fibers. The heat generated by the radiofrequency leads to the contraction of collagen, improving the skin's firmness and elasticity. Furthermore, the heating induces the activation of fibroblasts, leading to neocollagenization (altered in diameter, thickness and frequency), with subsequent tissue remodeling.
Keywords: PULSED RADIOFREQUENCY TREATMENT; COLLAGEN; SKIN AGING
With the increasing demand of patients for rejuvenation treatments and their intense desire to achieve this aesthetic improvement with minimal risk and a quick recovery, several non-surgical rejuvenation technologies have been developed. 1 A wide variety of high-tech devices are presented as effective, selective and safe therapeutic options.1
Traditionally, most non-surgical methods destroy the epidermis and cause dermal wounds, leading to the dermal remodeling of collagen, which causes the tightening of the skin, attenuating wrinkles. 1 Radiofrequency (RF) is a non-ablative, non-invasive rejuvenation method.
The electrical current produced by RF can reach deeper tissues, generating energy and strong heat due to the resistance present in the dermis and subcutaneous tissue. While a volumetric heating occurs on the inner layers of the skin, the surface is kept cooled and protected.
When heated, the collagen fibers denature and contract, resulting in the retraction of tissue. As the immediate contraction of the collagen fibers takes place with their shrinking, the formation of new fibers is stimulated (late neocollagenesis), increasing their efficiency in sustaining the skin. 2-5
Of all techniques based on the heating of the tissues, RF appears to be the most established and clinically proven, with the advantage of reaching the skin in its depth, due to the fact that even the hypodermis can be affected. 3 Therefore, Dermatology uses RF in a non-ablative way, promoting increased elasticity of tissues rich in collagen. 2
This source of energy and heat is defined as a radiation belonging in the electromagnetic spectrum (between 30KHz and 300MHz). 2 Many devices used in the day-to-day life, such as radios, televisions, wireless Internet, telephones, microwave ovens, satellite communications etc, operate based on RF. 2 Although the used energy (RF) is the same, different applications make use of different frequencies. 2 For medical and/or aesthetic purposes, RF frequencies above 10MHz are used. 2
Electrical currents have been used in medicine for more than a century, and in medical treatments for over 75 years, usually for minimizing the invasiveness of surgical procedures, while RF is used for ablation and coagulation procedures. 3
In aesthetic treatments, RF acts through its high-frequency current, which generates heat by conversion, deeply affecting tissular layers and promoting oxygenation, nutrition and vasodilation of the tissues; it acts by denaturing collagen fibers, resulting in their shortening and leading to the contraction of the redundant conjunctive tissue. 2, 3 When passing through the tissues, the current generates a slight friction (resistance of the tissues to the flow of RF), producing an increase in the local temperature. 2
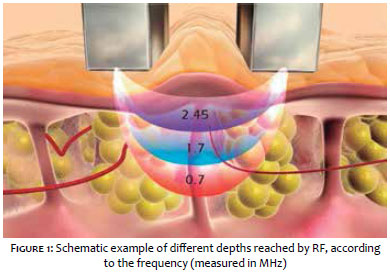
At the cellular level, the energy penetrates in the epidermis, dermis and hypodermis, also reaching muscle cells. It is worth to note that the RF's penetration depth is an inverse function of its frequency (Figure 1). 3
In July 2000, the US Food and Drug Administration (FDA) recognized the first RF system as a "non-invasive treatment for the attenuation of wrinkles and temporary improvement in the appearance of cellulite." This pioneering RF device was able to demonstrate its heating action up to the level of the papillary dermis and subcutaneous fat, leading to increased activity of fibroblasts and formation of new collagen (observed in a period that spanned months). With this, it was possible to clinically demonstrate the presence of significant contraction in the treated areas. 3 Since then many other RF devices have been developed, based on two main operating system types: unipolar (where the RF current flows through the body) and bipolar (where the RF current flow is limited to the volume located between the two electrodes). 3 Due to the fact that the use of the bipolar system is more localized, it usually requires less energy to achieve the same heating effect. 3
Several studies suggest RF as the gold standard noninvasive treatment leading to the retraction of the skin, demonstrating that the preservation of the skin's integrity minimizes the recovery and the risk of complications. 6_11
Many authors reported a significant attenuation of the sagging located in the neck and face of their patients, using scores to evaluate the clinical improvement and patient satisfaction.6-11
Other scientific publications attest to the safety of RF for treatments diverse from skin tightening, for instance in acne scars, skin rejuvenation and wrinkle reduction. 9 Its use in the palpebral area has also been proven safe, though it is deemed more effective when the defect is considered moderate. 12
Histological studies have evidenced the contraction of collagen fibers after treatment with RF, which led to a contraction in the tissue due to a mediate thermal stimulus, inducing the production of new collagen. 13 A number of studies monitored the action of the RF generated heat in the induction of collagen contraction, collagenesis and elastogenesis, with the resulting remodeling taking place during the treatment and for months after the application.14-17
While the effects of RF on the retraction of skin are undisputed, several studies describe limitations of this technology.14-17 The thermal effects of unipolar and bipolar RF were proven beneficial in skin tightening; nevertheless, they can be partial or unpredictable. 18
Up until a few years ago, the choices for treating sagging skin were strictly surgical. With the introduction of RF and other devices employing different energy sources used for shrinking tissue in a noninvasive manner, new options have emerged. However, these methods are limited by the recognized fact that the improvement of sagging skin can be difficult to achieve without the use of surgical procedures. 19 One hypothesis for the lack or unpredictability of the effectiveness of RF systems is the difficulty to adapt the power delivered to different individual skin impedances. 18
Adequate patient selection and the careful management of expectations are crucial, since the clinical results obtained with RF still have low predictability and reproducibility, and are not equivalent to those of plastic surgery.18,19 In this manner, defining the RF treatment as a rejuvenation, non-ablative technique that has action on the retraction and contour of moderately loose skin in patients without structural ptosis, will most likely lead to patient satisfaction regarding clinical outcomes.4, 5
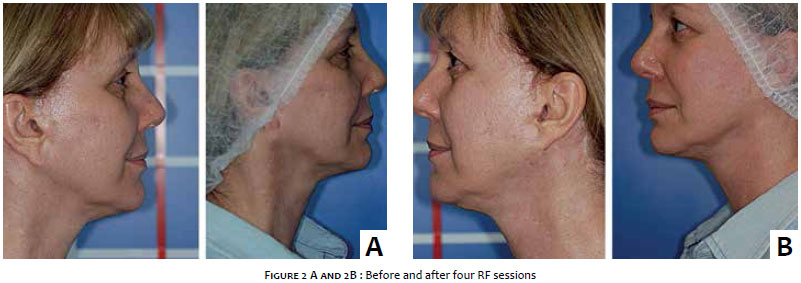
In these patients - and in those where avoiding surgical treatment modalities is desirable - RF offers a non-invasive alternative treatment based on the retraction of the skin and subcutaneous tissue, causing improvement in nasolabial lines and firmness in the jaw region, promoting the definition of the cervicomental angle, with absence of complications or need for recovery time.5, 20 (Figure 2)
In a clinical trial, almost 100% of patients experienced some degree of attenuation of sagging skin resulting from the treatment with a RF device. 21 (Figure 3) This study evidenced that patients often obtained visible results rapidly (within a week), however from a clinical point of view they became clinically more noticeable three months after the procedure, in general. 21 Other later phase studies have proven the presence of improvement three months after the treatment, with the follow up of patients being able to demonstrate even better results six months after the application of RF. 22 Despite the fact that it has been proved that effects of RF remain visible for six months after a single treatment, the longevity of clinical outcomes has yet to be determined.22, 23
Other studies are also concerned with the procedure's execution technique, for it can compromise the RF treatment's outcome. A greater increase in the temperature and its maintenance at around 40ºC throughout the duration of the application has the effect of reducing the extensibility and increasing the density of the collagen, entailing an improvement in the sagging of the skin. In RF, this effect is termed lifting. 2
There are many studies demonstrating the need to achieve a skin temperature of between 39ºC and 42ºC (clinically effective temperature) in order to obtain aesthetic effects with RF. 3 Aligned with this, devices and application techniques have been improved aiming at strengthening the RF's action. 24
The low frequency/multiple passes technique is an effective RF algorithm for skin tightening. 24 An evaluation of the multiple passes technique showed that all patients experienced some immediate erythema or edema, most of them completely resolved within 48 hours. There was absence of immediate abrasion or depigmentation in the 6 to 12-week follow up. 24 Photographic analyses of images obtained after the application with the multi passes technique confirmed the presence of visible esthetical improvement in facial and neck sagging in 96% of patients treated. 24
In another study, the application of monopolar RF on the face and neck using a vector multipass proved to be safe and tolerated by patients of all skin phototypes, with the patients' satisfaction being correlated with the images. 25
Stacked pulses in the submental region have also led to a reduction of fat.25 The reduction of fat is explained by the fact that, in addition to inducing collagen remodeling, the effects of RF heat also improve blood circulation. As a result, devices that use this source of energy produce electrothermal effects in the skin and subcutaneous tissue, which makes RF also indicated in all degenerative processes involving a reduction or delay of metabolism, irrigation and nutrition. 2, 3
The method causes vasodilation and increased irrigation beneath the treated area, as well as oxygenation and nutrition of the tissue. 2 With the increased circulation, a nutritional gain of oxygen, nutrients and trace elements takes place in the tissue. There is also an improvement in the cell residues (toxins and free radicals) drainage system. 2 These effects provide the opportunity to enhance the quality of adipocytes, causing homeostatic lipolysis and production of better quality elastic fibers. 2
When the body detects a temperature higher than the physiological level, capillary vessels open, causing vasodilation. In turn, this improves the tissular trophism and reabsorption of excess intercellular fluid, increasing blood circulation. 2 The heating effect also leads to an improvement in the microcirculation, resulting in the increase of blood flow to adipose tissues, which in turn causes an increase in the metabolism of the latter, homogenizing the subdermal fat and increasing the elasticity of the skin. 3 In theory, therefore, RF technology can be used not only in the reduction of sagging, but also in the reduction of body circumferences. 26
Franco et al. demonstrated that a ten-minute thermal exposure to 43ºC resulted in adipocyte cell death. In the same line of research, Galitzky et al. described an increase in the strength of fat cells lipolysis due to an increase in the catecholamines and blood flow. 3
Clinical studies have also demonstrated the effectiveness of RF in reducing localized fat and body contours, especially when combined with massage mechanisms or other technologies. 26
The use of better protocols and the combining RF with other technologies seem to be the future of the use of RF in dermatology. 5
Various RF based systems with aesthetic purposes (monopolar or bipolar, FDA approved) have emerged - some of them combining RF with other treatment modalities, such as infrared light, vacuum and mechanical massage - aiming at creating synergism in order to improve blood circulation and, consequently, the action of reducing body circumferences. 3, 27
The combination of RF and vacuum has been evaluated as safe and effective in several studies. In general, the vacuum mechanism makes an additional contribution to the penetration of the RF's energy in the skin. 3, 28
A histologic study of an area treated with RF associated to vacuum showed a decrease in the atrophy of collagen and an increase in the interstitial edema, indicating an improvement in dermal trophism. 3
The first RF device equipped with a vacuum unit has been described by Gold et al.. According to these authors, there was a significant improvement in the skin's appearance during the treatment and in a six-month follow up. 3 Montesi et al. reported clinical and histopathologic results using a bipolar device associated with vacuum for treating wrinkles, sagging skin, acne scars and stretch marks. 3
In many devices, the mechanical massage technique is used due to its direct effect on the microcirculation, providing improved lymphatic drainage and increased lipolysis. 3 Due to its action on the microcirculation, these devices are often used to treat cellulite. Although the therapeutic results of these technologies are apparently long-lasting, periodic applications are required to keep the achieved clinical outcomes.26, 29 There are reports in the literature on the use of non-invasive methods combining bipolar RF with other technologies, such as infrared light and massage mechanisms, for the treatment of cellulite, demonstrating that it can be significantly and safely reduced.26, 29
Isolated or associated with other methods, RF has few complications and has the additional advantage of allowing a prompt recover, with the patient returning to his or her daily routine immediately after the application4, 21 (Figure 4).
In the literature, reports of side effects were limited to transient erythema, edema and rare dysesthesias. 23 Studies performed with laboratory assessments of patients demonstrated that there were no alterations in the liver and/or lipid function indicators. 30 Ulcerations or pigmentation were not observed when the correct technique was applied, leading to the conclusion that RF heats the dermis and can achieve safe and effective tissue retraction. 21, 23
Even being considered a safe procedure, RF should be performed with moderate energy and without immediate overlapping in order to avoid overheating, leading to undesirable side effects. 31 Narins et al. described a rare case of over treatment of the tissue, leading to contour irregularities for more than six months that were later corrected with subincision and autologous fat. This side effect can be avoided asking for the patient's feedback on the feeling of warmth during the procedure. 3
There are few contraindications for the use of RF: pregnancy, use of electronic or metallic implant device, collagen or vascular disorders, active or recent malign disease, heat-stimulated disease, use of isotretinoin (controversial) and coagulopathy. It should not be applied over tattoos or permanent makeup. 3
It is important to note that, although it cannot be used during pregnancy, RF is a safe and effective method for reducing body circumferences and attenuate sagging skin in the immediate postpartum period. 32, 33
Radiofrequency is also safe when associated with other rejuvenation methods, such as a dermal implants. A study conducted with the application of RF two weeks after patients had undergone hyaluronic acid or calcium hydroxyapatite implants in the same area did not show any morphological alteration in the implanted material or surrounding skin. 34
In another study, patients were evaluated after having undergone dermal implants of hyaluronic acid in both sides of the face, followed by the application of RF in the same location, in only one of the sides. The side that received the dermal implant and the RF was compared to the contralateral side, which received only the hyaluronic acid implant. It was possible to observe that there were not histological changes after using the device over the area with the hyaluronic acid implant, leading to the conclusion that RF applied immediately and safely after the implantation of hyaluronic acid did not cause the reduction of the clinical effect or of other side effects. 35
A research conducted with pigs that were injected with different dermal fillers - human collagen (Cosmoplast), polylactic acid (Sculptra), liquid silicone (Silikon 1000), calcium hydroxyapatite (Radiesse) and hyaluronic acid (Restylane) - and subsequently treated with RF levels typically used in the daily practice, was designed to clinically and histologically evaluate changes occurred in the tissue. The filling substances injected were histologically analyzed five days, two weeks and one month after the treatment. Each of the fillers produced a specific inflammatory response, with no immediate thermal effect arising from the application of RF having been observed. On the other hand, the RF based treatment produced a statistically significant increase in inflammation, foreign body formation and fibrotic response associated with the fillers, which may be considered a positive effect of the combination of the two procedures. 36
Another association of methods evaluated was that of the use of RF technology after liposuction or laserlipolysis, aiming at increasing the skin's firmness and eliminating any irregularities after the removal of fat 3 (Figures 5 and 6).
In addition, devices that associate liposuction and RF on the same equipment have been positively evaluated for the reduction of significant amounts of fat, as well as for improving contours and effecting skin tightening. 37
In conclusion, RF is a method for the aesthetic treatment of the skin that has been developing rapidly since its inception, nearly two decades ago.
Both the application technique and the devices themselves have been going through advances, with other methods, such as massage and other technologies, having been incorporated in order to maximize outcomes in the treatment of sagging skin and body contours.
In practical terms, RF was proven effective for patients with good indication, bearing mild or moderate sagging. It has also showed action in the treatment of body contours and cellulite.
Some additional advantages of the method include a high level of safety, with few side effects having been reported, and the patient's ability to resume his or her routine immediately after undergoing the procedure. Its versatility should also be highlighted, for it can be used after other treatments, such as facial dermal implants or liposuction and its variations, in other body sites.
Despite the fact that its use can be limited in more severe cases, RF is, therefore, a widely used therapeutic method for the treatment of facial and corporeal skin sagging, as well as for improving body contours, with proven efficacy and a great level of safety.
1. Atiyeh BS; Dibo AS Nonsurgical nonablative treatment of aging skin: radiofrequency technologies between aggressive marketing and evidence-based efficacy. Aesthetic Plast Surg. 2009;33(3):283-94.
2. Carvalho, G F; Silva e col. Avaliação dos efeitos da radiofrequência no tecido conjuntivo. Rev Bras Med. 2011; 68(2 N. Especial). Acesso em: 10 out 2015. Disponível em: http://www.moreirajr.com.br/revistas.asp?id_materia=4555&fase=imprime
3. Inna Belenky e col. Exploring Channeling Optimized Radiofrequency Energy: a Review of Radiofrequency History and Applications in Esthetic Fields. Adv Ther. 2012;29(3):249-66.
4. Rusciani A; Curinga G; Menichini G; Alfano C; Rusciani L. Nonsurgical tightening of skin laxity: a new radiofrequency approach. J Drugs Dermatol. 2007;6(4):381-6, 2007.
5. Abraham MT; Vic Ross E Concepts in nonablative radiofrequency rejuvenation of the lower face and neck. Facial Plast Surg; 21(1):65-73.
6. Abraham MT; Mashkevich GFonte. Monopolar radiofrequency skin tightening. Facial Plast Surg Clin North Am. 2007;15(2):169-77.
7. Weiss RA; Weiss MA; Munavalli G; Beasley KL Monopolar radiofrequency facial tightening: a retrospective analysis of efficacy and safety in over 600 treatments. J Drugs Dermatol. 2006;5(8):707-12.
8. Koch RJ Radiofrequency nonablative tissue tightening.Facial Plast Surg Clin North Am. 2004;12(3):339-46.
9. Sadick N; Sorhaindo L. The radiofrequency frontier: a review of radiofrequency and combined radiofrequency pulsed-light technology in aesthetic medicine Facial. Plast Surg. 2004;21(2):131-8.
10. Fisher GH; Jacobson LG; Bernstein LJ; Kim KH; Geronemus RG. Nonablative radiofrequency treatment of facial laxity. Dermatol Surg. 2005;31(9 Pt 2):1237-41; discussion 1241.
11. Choi YJ; Lee JY; Ahn JY; Kim MN; Park MY The safety and efficacy of a combined diode laser and bipolar radiofrequency compared with combined infrared light and bipolar radiofrequency for skin rejuvenation. Indian. J Dermatol Venereol Leprol. 2012;78(2):146-52.
12. Carruthers J; Carruthers. A Shrinking upper and lower eyelid skin with a novel radiofrequency tip. Dermatol Surg2007;33(7):802-9.
13. Zelickson BD; Kist D; Bernstein E; Brown DB; Ksenzenko S; Burns J; Kilmer S; Mehregan D; Pope K Histological and ultrastructural evaluation of the effects of a radiofrequency-based nonablative dermal remodeling device: a pilot study. Arch Dermatol. 2004;140(2):204-9.
14. Paul M; Blugerman G; Kreindel M; Mulholland RS. Three-dimensional radiofrequency tissue tightening: a proposed mechanism and applications for body contouring. Aesthetic Plast Surg. 2011;35(1):87-95.
15. Sadick N Tissue tightening technologies: fact or fiction. Aesthet Surg J. 2008;28(2):180-8.
16. Collawn SSFonte. Skin tightening with fractional lasers, radiofrequency, Smartlipo Ann Plast Surg. 2010;64(5):526-9.
17. Goldberg DJ. Nonablative laser technology Radiofrequency. Aesthet Surg J. 2004;4(2):180-1.
18. Harth Y; Lischinsky D A novel method for real-time skin impedance measurement during radiofrequency skin tightening treatments. J Cosmet Dermatol. 2011;10(1): 24-9.
19. Dierickx CCFonte. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg Med. 2006;38(9):799-807.
20. Hassun, K.M; Bagatin, E. Ventura, K. F. Radiofreqüência e infravermelho: [revisão] Rev Bras Med. 2008;65(N. Especial):18-20.
21. Ruiz-Esparza J; Gomez JB. Medical face lift: a noninvasive, nonsurgical approach to tissue tightening in facial skin using nonablative radiofrequency. Dermatol Surg. 2003;29(4):325-32.
22. Kushikata N; Negishi K; Tezuka Y; Takeuchi K; Wakamatsu S.Non-ablative skin tightening with radiofrequency in Asian skin. . Lasers Surg Med. 2005;36(2):92-7.
23. Alster TS; Tanzi E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: a lifting experience Dermatol Surg. 2004;30(4 Pt 1):503-7.
24. Bogle MA; Ubelhoer N; Weiss RA; Mayoral F; Kaminer MS. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39(3):210-7.
25. Finzi E; Spangler A. Multipass vector (mpave) technique with nonablative radiofrequency to treat facial and neck laxity. Dermatol Surg. 2005;31(8 Pt 1):916-22.
26. Hexsel DM; Siega C; Schilling-Souza J; Porto MD; Rodrigues TC. A bipolar radiofrequency, infrared, vacuum and mechanical massage device for treatment of cellulite: a pilot study. J Cosmet Laser Ther. 2011;13(6):297- 302.
27. Gold MH. Tissue tightening: a hot topic utilizing deep dermal heating. J Drugs Dermatol. 2007;6(12):1238-42.
28. Gold MH; Goldman MP; Rao J; Carcamo AS; Ehrlich M.Treatment of wrinkles and elastosis using vacuum-assisted bipolar radiofrequency heating of the dermis.: Dermatol Surg. 2007;33(3):300-9.
29. Alster TS; Tanzi EL. Cellulite treatment using a novel combination radiofrequency, infrared light, and mechanical tissue manipulation device . J Cosmet Laser Ther. 2005;7(2):81-5.
30. Levenberg A Clinical. Experience with a TriPollar radiofrequency system for facial and body aesthetic treatments. Eur J Dermatol. 2010;20(5):615-9.
31. de Felipe I; Del Cueto SR; Pérez E; Redondo P: Adverse reactions after nonablative radiofrequency: follow-up of 290 patients. J Cosmet Dermatol. 2007;6(3):163-6.
32. Brightman L; Weiss E; Chapas AM; Karen J; Hale E; Bernstein L; Geronemus RG Improvement in arm and post-partum abdominal and flank subcutaneous fat deposits and skin laxity using a bipolar radiofrequency, infrared, vacuum and mechanical massage device. Lasers Surg Med. 2009;41(10):791-8.
33. Winter ML. Post-pregnancy body contouring using a combined radiofrequency, infrared light and tissue manipulation device. J Cosmet Laser Ther.2009;11(4):229-35.
34. Alam M; Levy R; Pajvani U; Pavjani U; Ramierez JA; Guitart J; Veen H; Gladstone HB Safety of radiofrequency treatment over human skin previously injected with medium-term injectable soft-tissue augmentation materials: a controlled pilot trial. Lasers Surg Med. 2006;38(3):205-10.
35. Goldman MP; Alster TS; Weiss R. A randomized trial to determine the influence of laser therapy, monopolar radiofrequency treatment, and intense pulsed light therapy administered immediately after hyaluronic acid gel implantation. Dermatol Surg. 2007;33(5):535-42.
36. Shumaker PR; England LJ; Dover JS; Ross EV; Harford R; Derienzo D; Bogle M; Uebelhoer N; Jacoby M; Pope K. Effect of monopolar radiofrequency treatment over soft-tissue fillers in an animal model: part 2. Lasers Surg Med. 2006;38(3):211-7.
37. Hurwitz D; Smith D Treatment of overweight patients by radiofrequency- -assisted liposuction (RFAL) for aesthetic reshaping and skin tightening Aesthetic Plast Surg. 2012;36(1):62-71.
The present study was carried out at the author's private practice in Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}