


Priscila Regina Orso Rebellato1; Luciana Rodrigues Lisboa Faucz2; Juliano Vilaverde Schmitt3; Camila Araújo Scharf Pinto4
Introdução: actinic melanosis is a pigmentation disorder caused by the cumulative action of sunlight on the skin and its incidence increases with advancing age. Objective: Considering the lack of studies comparing agents with the same concentration, however in different vehicles, the authors compared the clinical effects of chemical peelings performed with 20% trichloroacetic acid (ATA) paste or solution in the treatment of actinic melanoses in the back of the hands. Methods: A prospective, controlled, randomized study was carried out with 15 patients bearers of bilateral actinic melanoses on the back of the hands. Three monthly sessions with 20% ATA peelings were performed with paste in one hand and solution in the other. The degree of whitening was evaluated by 13 blinded dermatologists, and patients were asked about the satisfaction and preferred method. Results: There was no preference for any of the methods used (p = 0.41), however, according to the medical evaluation, there was greater whitening with the paste (p = 0.01). Only the paste caused significant adverse effects, affecting 4/15 patients. Conclusions: Compared to the solution, when applied for two minutes in the treatment of actinic melanosis, the 20% ATA paste had greater whitening capacity, however demonstrated a tendency to cause more local adverse effects.
Keywords: TRICHLOROACETIC ACID; MELANOSIS; HAND; CHEMEXFOLIATION; SKIN PIGMENTATION
In a study conducted by the Brazilian Society of Dermatology, pigmentation disorders were the most frequent causes of visits to dermatological practices among patients aged 40-64 years. 1 Actinic melanosis (AM), or solar melanosis, is a common skin disorder among these dermatological complaints, originating from the cumulative action of sunlight on the skin after the third or fourth decades of life.2, 3
In addition to the effective and regular protection against the sun, treatment of melanoses includes topical medications with lightening effect and ablative procedures such as cryotherapy, laser, intense pulsed light and localized application of caustic liquids such as trichloroacetic acid (TCA) and phenol. The application of caustic agents in the form of chemical peelings on the dorsum of the hands is also reported in the treatment of solar melanosis. A more diffuse application of the caustic agent in the affected region has the additional effect of treating incipient or sub-clinical lesions, as well as other aspects of photoaging often associated with solar melanosis. 4, 5
Despite the availability of a number of options for the treatment of solar melanosis, there are few studies comparing techniques.
The use of TCA for performing chemical peels have been reported mainly in two vehicles: aqueous solution and water-soluble paste.
In general, the TCA peeling in aqueous solution is carried out in successive applications, interspersed with standardized time intervals after which the level of the inflicted damage (frosting) caused by prior applications is checked. 6
The TCA paste was created with the purpose of obtaining greater uniformity in the acid's effect. Pastes are semisolid consistency pharmaceutical preparations that contain a significant proportion of insoluble solid particles (~20-50%), and are formulated with excipients of oily or aqueous characteristics. 2
The rheological characteristics of the pharmaceutical preparations interfere with the speed of release of the active principle, in speed of evaporation of the solvent and in the amount of the active principle applied per area of skin.
In the present study, the authors compared the efficacy and safety of TCA (paste and solution) in the treatment of solar melanosis in the dorsum of the hands.
A prospective, controlled, randomized, clinical trial was performed with 15 selected patients who bore at least five AM lesions on the dorsum of the hands and sought care at the Dermatology Ambulatory of the Hospital Universitário Evangélico de Curitiba (Curitiba, Paraná State, Brazil).
The exclusion criteria were: individuals with previous or current history of warts or recurrent herpes in the dorsum of the hands; pregnant women or nursing mothers; patients with active skin infection in the site of application the peeling; history of hypersensitivity to TCA, sunburn in the previous three days, surgery, cryotherapy, radiation therapy or PUVA in the previous six weeks; patients under systemic use of isotretinoin in the previous six months; and patients unable to understand the post-peeling care instructions or who were unable to complete the study.
The TCA solution was prepared only in demineralized water, and the base paste for the TCA contained the following components: glycerin, sorbitol, talc, aerosil, Veegum k, blanc covasop, phenonip and water. The concentration of TCA was titled at 20% of solute mass / solution mass for both formulations.
Three peeling sessions were performed with 30-day intervals. Before the application, the dorsa of the hands were degreased with 70% alcohol. In a random manner, the dorsum of one hand was treated with 20% TCAA solution and the other with 20% TCA paste. The preparation type chosen in the first session was applied to the same hand in the following two sessions. The application of the paste was performed with a spatula, leaving the product in contact with the skin for two minutes, with the application site being washed thoroughly with 0.9% saline until complete removal. The solution was applied in layers with a moistened gauze until the appearance of level II frosting (white uniform cover with a bright pink background), without rinsing. The patients were instructed not to wash their hands in the following three hours after the application and to use liquid petrolatum in the application site during the following five days. They were also instructed not to get exposed to the sun and apply sunscreen daily. Both the sunscreen and the liquid petrolatum were standardized and provided.
The degree of lightening of the lesions was evaluated by 13 dermatologists through photographs taken before and 30 days after the end of treatment, without identifying the method used. The level of improvement was evaluated according to a semiquantitative scale ranging from 0 to 3 (0 - Absence of improvement/whitening <25%, 1 - Slight improvement/whitening 25-50%, 2 - Moderate improvement/whitening 50-75%, 3 - Significant improvement/whitening >75%).
Finally, the degree of satisfaction of each patient regarding each treatment was evaluated by using a scale with three choices: unsatisfied, somewhat satisfied and satisfied.
The research project was approved by the Research Ethics Committee of the institution, and all participants read and signed a free and informed term of consent.
The categorical data were represented by proportions and absolute numbers, while the parametric data was represented by mean values ± standard deviation. The Binomial, Fisher exact and Mann-Whitney tests were used, as well as the intraclass correlation (absolute agreement). The generalized linear mixed model with gamma type curve adjustment was used for the analysis of the scores attributed by the dermatologists. The data were analyzed using the IBM SPSS 20 software, with values being considered significant when p<0.05.
Fifteen (15) female patients were included, of which four (4) had significant adverse effects with the paste, and none had adverse effects with the solution (p = 0.10 - Fisher's exact test). One (1) patient did not complete the study due to an intense irritation in the site of application of TCA paste, with the formation of blisters. Two (2) patients had severe burning sensation during the application of the paste, occasioning a reduction in the time of action to 1.5 minute in the following sessions, with good development. One (1) patient had pustules after the first session on the hand that received paste, with the picture being resolved with systemic antibiotic and topical corticosteroid of medium potency for seven days, without recurrence in the following sessions. In this manner, 14 women completed the study, of which nine (9) had skin phototype II and five (5) phototype III, and a mean age of 58 ± 10.7 years.
Of these 14 women, none was unsatisfied with both treatments, with 12 having been very satisfied with the paste and 11 very satisfied with the solution (p = 0.99 - Fisher's exact test). Regarding the preference for the methods, 5 preferred the paste and 8 the solution (p = 0.41 - binomial test).
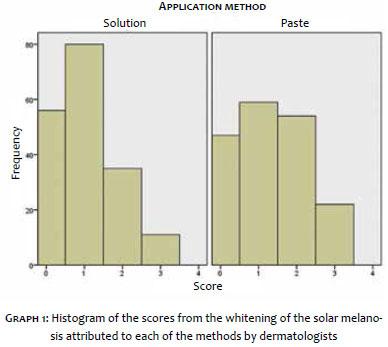
Regarding the assessment of the dermatologists, there was satisfactory intraclass correlation (0.87) among the 13 evaluators, with the mean score of the clinical improvement attributed to the paste being greater than that attributed to the solution (1.28 ± 0.98 x 1.01 ± 0.86, p = 0.01 - Mann-Whitney test) (Figures 1 and 2) (Graph 1). The superiority of the paste was later confirmed by a generalized linear mixed model controlled by the variables evaluator dermatologist, patient and treated limb (p <0.01; Coefficient = 0.11 [IC 95%: 0.04 to 0.18]; Akaike = 361.5; Bayesian = 413.6).
TCA has been used in the ablative treatment of solar melanosis with satisfactory results. 7 It is a chemical cautery that coagulates skin proteins and can be used localized points or in the form of chemical peels. 8
The depth of the caustic effect is determined by the following factors: thickness and degree of oiliness of the target skin, concentration of the active substance, degree of previous degreasing, friction during application, occlusion and the volume applied.1, 9, 10 Furthermore, there are different preparations that, due to their physico-chemical properties, convey the active principle to the site of action in different ways.
According to literature review performed by the authors, there is absence of studies comparing the application of peelings using different vehicles. On the other hand, some studies compare cryotherapy with 33% to 40% TCA peeling in the treatment of solar melanosis with results favorable to the first method. 11-13
In the present study, from the patients' point of view, none of the methods stood out regarding preference or satisfaction. On the other hand, in the blind evaluation of the aesthetic result carried out by dermatologists, the use of the paste was significantly superior.
Despite the fact that the dermatologists' evaluations have shown a higher degree of whitening with the paste formulation, it is worth to note that the adverse effects with this vehicle tended to be more intense.
The TCA paste's opacity hampers the assessment of the level of damage (or frosting), caused by the active principle, making it difficult to identify the appropriate instant to remove the caustic agent. On the other hand, defining a fixed exposure time to the acid disregards the variability of the response to the product among individuals.
In their study, Goldust M. et al. found hyperpigmentation was the main adverse effect to the use of TCA, however the concentration of the acid used was 40%, the vehicle was the aqueous solution, and it was applied punctually on each of the lesions caused by the sun. Unlike in the present study, where a lower concentration was used and paste applied diffusely, there were no cases of hyperpigmentation or any additional long-term effect.
Peelings using a solution or paste containing 20% TCA to treat actinic melanosis in the dorsum of the hands were proven efficient. The duration of the exposure to the paste, set at two minutes, seems to provide an effective whitening effect that is superior to that resulting from the use of the solution, the latter limited to a level II frosting. On the other hand, the paste's caustic action intensity is relatively erratic, with one quarter of the patients presenting significant adverse effects.
Setting a standard time of exposure to the TCA paste might prove not to be an adequate approach while objective factors that can predict individual susceptibility to its harmful effects have not been identified by further studies.
1. Sittart JAS, Zanardi FHT. Prevalência das dermatoses em pacientes da 4ª idade. Rev Soc Bras Clin Med. 2008;6(4):125-9.
2. Machado Filho CDS, Meski APG, Grinblat BM, Garrone MH. Discromias. In: Belda Junior W, Di Chicaccio N, Criado PR. Tratado de Dermatologia. São Paulo: Atheneu; 2010. p. 667-91.
3. Sampaio SAP, Rivitti EA. Dermatologia. São Paulo: Artes Médicas; 2007. p. 353-74.
4. Miot LDB, Miot HA, Silva MG, Marques MEA. Fisiopatologia do melasma. An Bras Dermatol. 2009;84(6):623-35.
5. Costa IMC. Peelings químicos. In: Lupi O, Belo J, Cunha PR. Rotinas de diagnóstico e tratamento da Sociedade Brasileira de Dermatologia. 2.ed. Itapevi: AC Farmacêutica; 2012. p. 496-502.
6. Zanini M. Gel de ácido tricloroacético: uma nova técnica para um antigo ácido. Med Cutan Iber Lat Am. 2007;35(1):14-7.
7. Bagatin E. Peelings químicos corporais. In: Kadunc BV, Palermo E, Addor FAS, Metsavaht LD, Mattos R, Bezerra SMC. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 327-32.
8. Kadunc BV. Introdução aos peelings químicos. In: Kadunc BV, Palermo E, Addor FAS, Metsavaht LD, Mattos R, Bezerra SMC. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012.p. 311.
9. Kede MPV. Peelings químicos. In: Ramos-e-Silva M, Castro MCR. Fundamentos de Dermatologia. Rio de Janeiro: Atheneu; 2009. p. 2247-68.
10. Yokomizo VMF, Benemond TMH, Chizaki C, Benemond PH. Peelings químicos: revisão e aplicação prática. Surg Cosmet Dermatol. 2013;5(1):58-8.
11. Goldust M, Golforoushan F, Sadeghi M, Rezaee E. A comparative study in the treatment of Solar Lenigines with Trichloroacetic Acid 40% versus Cryotherapy. Cosmetic Dermatol. 2011;24(5):215-9.
12. Golforoushan F, Azimi H, Sadeghi M, Yousefi N, Goldust M. Efficacy and side effects os Trichloroacetic Acid (TCA) versus Cryotherapy in the treatment of solar lentigo. Iranian J Dermatol. 2010;13(52):47-51.
13. Raziee M, Balighi K, Shabanzadeh-Dehkordi H, Robati RM. Efficacy and safety of cryotherapy vs. trichloroacetic acid in the treatment of solar lentigo. J Eur Acad Dermatol. 2008;22(3):316-9.
The present study was performed at the Hospital Universitário Evangélico de Curitiba - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}