


Tassiana Simão1; Mônica J. Mateus Tarazona2; Paula Renaux3; Roberto Souto4; Luna Azulay5; João Carlos Macedo Fonseca6
Ascher syndrome (AS) is a rare disorder of unknown etiology characterized by the presence of double upper lip, blepharochalasis and nontoxic goiter (complete AS). The nontoxic goiter is present in 10-50% of cases (incomplete AS). Trauma, hormonal dysfunction, autosomal dominant inheritance, defects in elastic fibers and allergy are possible causes. Surgery is indicated due to the compromise of facial aesthetics, trauma, or visual difficulty, and to restore the patient's quality of life. The present article reports the case of a patient with a double and blepharochalasis lip, diagnosed as a bearer of the incomplete Ascher syndrome, and describes the adopted conduct.
Keywords: BLEPHAROPLASTY ; BLEPHAROPTOSIS; LIP
The Ascher's syndrome is a rare, benign entity of unknown etiology. Since it was described up until the present time, just over 50 cases were described in the literature. 1 It is clinically characterized by the triad double upper lip, blepharochalasis and nontoxic goiter, which compose the complete form of the syndrome. 2 However, the nontoxic goiter is present in only 10% to 50% of cases, and its presence is not essential for diagnosis (incomplete Ascher's syndrome). 2,3 In this article, the authors report the case of a patient bearing double lip with blepharochalasis, diagnosed with incomplete Ascher's syndrome, describing the adopted approach.
A 15 year-old male patient sought care at the Dermatology Department of the Hospital Universitário Pedro Ernesto da Universidade do Estado do Rio de Janeiro (RJ), Brazil, with a history of fixed edema in the upper lip for about five years, and recurrent edema in the upper eyelids for one year, with worsening after exposure to the sun. The patient did not report history of previous trauma, surgery or illnesses. There is no similar family history.
The dermatological examination evidenced the presence of blepharochalasis in the upper eyelid bilaterally, which was pseudoptotic, with loose skin and a local crease reaching the eyelashes level, making difficult the complete opening of the eyes (Figure 1). The presence of double upper lip was also observed with increased volume and a transversal groove (Figure 2). Laboratory tests (blood count, blood glucose, liver and kidney function, thyroid stimulating hormones, free T4, antithyroid antibodies), as well as the ultrasound examination of the thyroid came out normal. Also, a labial lesion biopsy was carried out yielding no relevant findings. The patient was then clinically diagnosed with the Ascher's syndrome.
Surgical technique
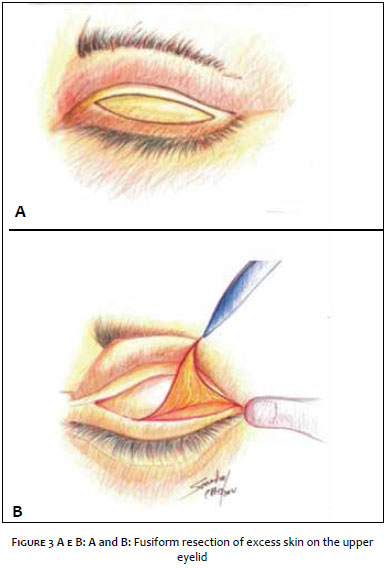
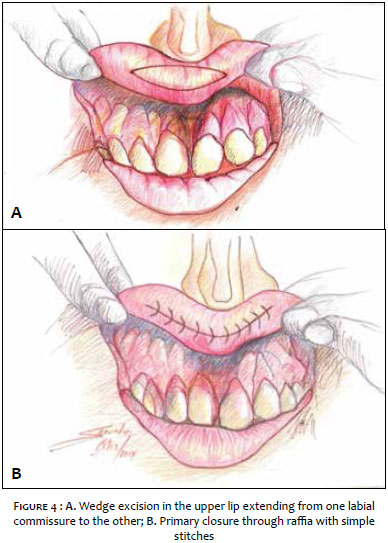
The patient used 2g of antibiotic prophylaxis one hour before (Amoxil®, GlaxoSmithKline, London, UK) and was underwent the surgical procedure after asepsis and antisepsis (Marcodine®, Cristália, Itapira, SP, Brazil). Infraorbicular and Intraoral mentonian anesthetic block and palpebral infiltrative anesthesia with 2% lidocaine hydrochloride (Hypofarma, Ribeirão das Neves, MG, Brazil), were carried out. A fusiform resection of the excess skin was performed on the upper eyelid (Figure 3), followed by hemostasis and primary closure with interrupted stitches (Prolene® 6-0, Ethicon, Somerville, NJ, USA). The excess skin in the upper lip was treated with a wedge excision, extending from one labial commissure to the other, followed by local hemostasis and subsequent primary closure with simple stitches (Chromic Catgut® 4-0, Ethicon, Somerville, NJ, USA) (Figure 4). The removal of the stitches was performed seven days after the surgery. The patient progressed with good local healing (Figures 5 and 6).
The Ascher's syndrome is classified as an anetoderma subtype. 1 It was initially described in its complete form by the Austrian ophthalmologist K. W. Ascher in 1920. One year later, Weve described the syndrome with the inconstant presence of goiter, characterizing the complete form. 2, 3
Studies show that only 10% of blepharochalasis cases in young patients are associated with double lip. 2 The labial and palpebral involvement usually occurs concomitantly, and in over 80% of cases the condition emerges before 20 years of age. 1, 2
The cause of the syndrome is still unknown, though factors such as trauma and hormonal dysfunction have been implicated as possible etiologies. 1, 2, 4 Some authors cite dominant autosomal heritage, allergy, defects in elastic fibers, which seem to be fragmented or reduced in size.1 Double lip or macrocheilia can be congenital or acquired, 2 and the simultaneous involvement of the upper and lower lips is a common finding. However it can occur isolatedly, with an incidence of 10:1 of involvement of the upper lip. It is characterized by an alteration of the labial mucosa, without involvement of the muscles. 5, 6
The acquired type generally results from local trauma, whereas the congenital type results from a development anomaly, and may be associated with bifid uvula, palatine fissure, glandular cheilitis and hemangioma. 2, 4, 7-9
During the embryonic period, the upper lip consists of two transversal zones: an external cutaneous zone (pars glabra) and an internal mucosa zone (pars villosa). 2 The glandular hypertrophy of the pars villosa forms a line along the boundary between these two structures, delimiting the transversal groove from the labial duplicity. 2, 4 The internal portion of the lip (pars villosa) usually remains beneath the external portion (pars glabra), and when the patient smiles, there is compression of the lip against the teeth, giving the impression of presence of double lip, with two borders in the vermilion. 2 Thus, although the deformity may already be present at birth, it only becomes apparent after the final eruption of teeth. 1, 2 In the case of interference in the speaking or chewing functions, or due to patients' esthetical desire, surgical treatment is indicated, so as to resect the transversal groove. 3, 4, 6
Blepharochalasis is characterized by progressive atrophy and relaxation of the skin, with prolapsed orbital fat and fall of the affected eyelid. 1 Visual alterations may occur due to the narrowing of the palpebral fissure. 1 Recurrent edema can be present and worsen the picture. 2 A certain degree of blepharochalasis linked to the atrophic skin and the relaxation of the eyebrows is common in aging, but uncommon in young people, characterizing a disorder in the elastic tissue, such as the lax skin, or have idiopathic origin 1, 8 The crucial differentiation between the Ascher's syndrome and the blepharochalasis is carried out through histology, when the absence or small amount of elastic fibers is evidenced in the affected tissue, associated with atrophic skin in the second condition. 1 On the other hand, the nontoxic goiter is inconstant, present in about 10% to 50% of cases, and can emerge several years after the labial and palpebral involvement. 2, 5
In the present case, there was no evidence of involvement of the thyroid gland at diagnosis, characterizing the incomplete form of the syndrome.
As mentioned, the appropriate therapeutic approach instituted for this patient was surgery, through resection of the skin, along the lines of conventional blepharoplasty and a transversal elliptical labial incision, thus correcting the macrocheilia.
In this way, when the clinical findings and the patient's history lead to the initial diagnosis of double lip, it must be considered both in isolation or as part of the Ascher's syndrome, aiming at performing a diagnostic investigation and instituting the proper treatment.
Therefore, due to the compromise of the patient's facial aesthetics, frequent traumas, increased volume of the lips, and visual impairment, the surgical intervention is indicated in both cases. The surgery should be performed in face of clinical complaint, usually showing good development, with relevant improvement in aesthetics and function, in this way returning quality of life to the patient.
1. Cruz G, Freitas RS, Bertollote W, Santos AR. Síndrome de Ascher: aspectos clínicos e terapêuticos desta rara deformidade da face. Rev Bras Cir Craniomaxilofac 2008;11(3):116-8.
2. Eidt G, Dos Santos M, Sartor S, Neto L. Síndrome de Ascher, relato de caso do projeto diagnóstico bucal do curso de odontologia da Universidade de Santa Cruz do Sul. Anais III Salão de Ensino e de Extensão 2011;341.
3. Azenha MR, Marzola C, Pereira LC, Brandt Júnior SHO. Lábio duplo de origem congênita relato de caso e técnica cirúrgica. Rev Bras Odontol. 2007;64(3-4):152-4.
4. Carraro R, Pacheco A, Zanardi D, Filho J. Você Conhece Esta Síndrome?. An Bras Dermatol. 2006;81(3):281-9.
5. Hanemann JA, Oliveira DT, Gomes MF, dos Anjos MJ, Sant'ana E. Congenital double lip associated to hemangiomas: report of a case. Med Oral. 2004;9(2):156-8, 155-6.
6. Barnett ML, Bosshardt LL, Morgan F. Double lip and double lip with blepharocalasis (Ascher's syndrome). Oral Surg Oral Med Oral Pathol. 1972;34(5):727-33.
7. Brinhole MCP, Real DG, Giovani EM, Costa C, Armonia PL, Melo JAJ, et al . Lábio duplo congênito. Rev Inst Ciênc Saúde. 2006;24(4):327-30.
8. Calnan J. Congenital double lip: Record of a case with a note on the embryology. Br J Plast Surg. 1952;5(3):197-202.
9. Cohen DM, Green JG, Diekmann SL. Concurrent anomalies: cheilitis glandularis and double lip. Oral Surg Oral Med Oral Pathol. 1988;66(3):397-9.
The present study was conducted at the Hospital Universitário Pedro Ernesto da Universidade do Estado do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}