


Patrick Alexander Wachholz1; Paula Yoshiko Masuda2; Christiane Salgado Sette3
Hansenomas originate from the intense cutaneous infiltration by Mycobacterium leprae bacilli in Virchowian hansenic patients who tend to improve with treatment,however can develop keloid reactions. Alternative approaches are described for the treatment of disseminated receding hansenomas in the ears, face, upper limbs, and trunk in already treated virchowian patients. The exeresis of the lesion in the left ear was carried out and followed by injections of triamcinolone in the surgical scar, combined with simple injections in other lesions in exposed areas and an expectant approach in other areas. A good cosmetic result was observed in the excised lesion, in addition to a reduction in the lesions injected with corticosteroids. These procedures are easy to perform and cost effective, yielding good aesthetic outcomes.
Keywords: LEPROSY; LEPROSY, LEPROMATOUS; MYCOBACTERIUM LEPRAE; THERAPEUTIC USES
The pathophysiology of the Hansen's disease manifestations is related to the immune response of the host, to complications of peripheral neurologic involvement and to cellular/tissular damage secondary to the multiplication and dissemination of bacilli. 1 In the anergic pole of the disease, the absence of cellular immunity against Mycobacterium leprae in patients with Virchowian hanseniasis (VH) triggers characteristic clinical manifestations due to the infiltration of the bacilli throughout the skin's depth. 2
When the bacillary infiltration is intense, a polymorphism of lesions can be observed, including papules, tubercles, nodules, diffuse infiltration and ulcerations, in addition to cutaneous plaques termed hansenomas. 2 The hansenomas usually only spare axial regions (vertebral spine, Michaelis' polygon) and body areas with higher temperature, such as the groin, axillary and regions, and popliteal cavus. 2
With the establishment of multibacillary polychemotherapy (Mb-PCT), the hansenomas tend to regress spontaneously. 2, 3 In exceptional cases, however, they may persist (hansenomas in regression) or develop with fibroblast proliferation and keloidal reactions. 3 Descriptions of the management of these lesions in patients with VH are extremely rare in the literature. 1, 4, 5
The correct diagnosis of lesions suggestive of hansenomas is crucial for the latter constitute a potential source of contagion in case there are viable bacilli. Furthermore, the presence of volumous lesions or a great number of lesions significantly undermines the quality of life and contributes to the stigmatization of patients.2, 6, 7
The present report describes and reviews different techniques and discusses evidences of potential therapeutic alternatives for hansenomas in regression associated with keloidal reaction in a patient with treated VH.
A 52 year-old male patient from the Brazilian Southeast Region seaside town of Itanhaém (SP) was diagnosed with VH at another dermatologic care service in the first half of 2009. He received Mb-PCT for 24 months due to high bacillary quantity and great number of hansenoma type cutaneous lesions. There was absence of record of dapsone based monotherapy, and the patient denied cutaneous trauma or acne. At the end of the Mb-PCT, few hansenomas had regressed. He was referred to a tertiary dermatologic service in July 2013 for evaluation of the possibility of drug resistance or disease activity.
On admission, the patient had a great number of erythematous nodular, hyperchromic and painless lesions, in the face, ears, chest, abdomen and upper limbs (Figure 1 A-D). He had reduced strength and sensation in the hands and acrocyanosis. In the face of lesions suggestive of hansenomas in patients who have already undergone Mb-PCT, it is imperative to consider differential diagnoses: 2, 3 the most likely causes included active hanseniasis, histoid leprosy, drug resistance or insufficient treatment.2
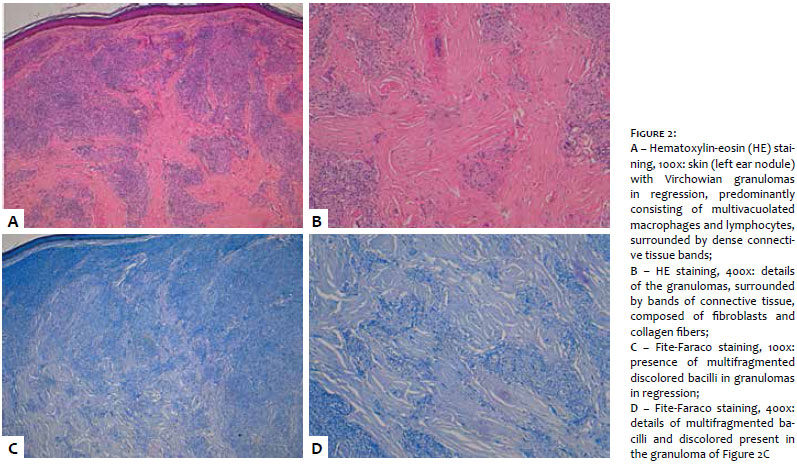
The biopsy revealed hansenoma in regression, with histiocytes containing multifragmented bacilli, slightly colored/discolored, permeated by lymphocytes and plasmocytes, with dermal stromal proliferation of the hypertrophic scar/keloid type forming hyalinized collagen bands (Figures 2 A-D). The bacilloscopy came out positive, with a bacillary index of 2.34, a morphological index of 0, and a reagent PGL-1 test. Inoculation into footpads of nude mice for phenotypic analysis of drug resistance showed absence of bacterial multiplication. The diagnosis was: treated VH with presence of hansenomas in regression associated with fibroblast proliferation of the keloidal type.
Due to the unsightly nature of lesion in the left ear (Figure 1D), the great number of residual lesions in the trunk and exposed areas (Figures 1 A-B), and to the lack of evidence of the effectiveness of alternative therapies for such unusual lesions, three different types of interventions were proposed and consented by the patient.
The decision in favor of comparing the results in the same patient was aimed at not only avoiding lengthy procedures - which were unlikely to recover the aesthetics idealized by the patient - but also empirically assessing the superiority of the modalities from the patient's and the team's subjective opinion.
The surgical excision of the lesion in the left ear was carried out, followed by triamcinolone injections in the surgical scar. In the hansenomas located in exposed areas (face and upper limbs) only injections of corticosteroids were performed. An expectant approach was adopted in the other lesions.
The lesion in the earlobe was pedunculated due to local skin laxity. The technique included the marking of the lesion, anesthesia with 2% lidocaine, fusiform incision, detachment in layers, preparation of the flap by sliding the margins, and simple suture with nylon 6.0 monofilament. The stitches were removed on the 9th postoperative day, with two injections having been carried out in 30-day intervals, with 20mg/ml triamcinolone hexacetonide at a dose of 0.2 ml per injection.
In the lesions located in the face and upper limbs, two sessions of intralesional corticosteroid injections with the same substance were applied in each lesion, at a dose of 0.8 ml per session, observing the same time interval between sessions. The lesions located in the trunk were only monitored during the follow-up period.
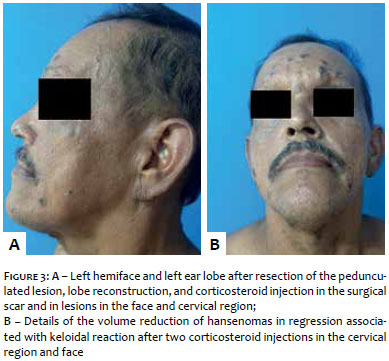
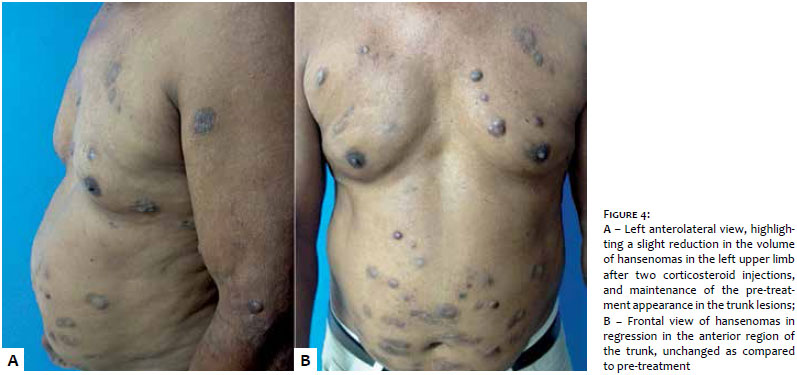
Six months after it was possible to observe an excellent aesthetic result in the lesion located in the ear, without recurrence (Figure 3 A-B). The lesions that received injections had mild to moderate reduction (Figure 4 A-B). The lesions that were under expectant approach remained unchanged. The patient's and team's perception of improvement was considered very good.
Despite having considered the possibility of histoid leprosy, this variety manifests with intensely bacillary lesions with the predominance of typical bacilli, potentially resistant to therapy. 1, 5 The nodules' appearance is different, with well delimited, skin-color bright lesions, usually firm and translucent, with histology displaying numerous fusiform histiocytes and polygonal cells arranged in a crossed or intertwined characteristic spiral. 1-3, 5
In the face of a hansenoma in regression with keloidal type reaction diagnosis, it is important to consider potential alternative therapies aimed at easing the disease's stigma.
The available evidence on the management of hypertrophic and keloid scars (not specifically related to leprosy) has been revised in recent years. 8-10 Treatment strategies are largely determined by the lesion's classification, 8 and include silicone-based products, intralesional corticosteroids, 5-fluorouracil and intralesional bleomycin, radiotherapy, cryotherapy 8-10 in addition to emerging treatment with mitomycin-C, imiquimod and onion extracts and heparin, 8, 10 as well as interventions and surgical laser. 8-10
Due to the high number of lesions, a decision was made in favor of injecting only the more exposed lesions. Corticosteroids injections is a well established option due to the drug's collagenesis inhibitory property, increasing the alpha-2 macroglobulin and alpha-1 antitrypsin, leading to decreased synthesis of collagen. 5 Intralesional corticosteroids is described as the first choice in keloids by some authors, 8,10 despite the fact that others recommend the previous use of silicone-based products (sheets or gel). 9
The use of intralesional corticosteroids is also associated to the lower recurrence rate after surgical removal. 8 Despite the small number of studies and the absence to date of randomized trials comparing the efficacy of these therapeutic modalities, promising studies have been published on the use of 5-fluorouracil intralesionally, isolatedly or in association with corticosteroids, especially in patients with high recurrence rates after excision. 8, 9 Similarly, studies on the use of bleomycin are promising, however they lack validation, including safety analysis, due to the higher risk of hyperpigmentation and cutaneous atrophy. 10 The first publications featuring topical mitomycin-C are also contradictory, indicating a possible advantage in the reduction of recurrence after surgical removal of the lesions, nevertheless with increased risk of ulceration. 8
The results observed in the development of the present case demonstrated that the procedures adopted, in addition to being cost effective, easy to implement and with good aesthetics and functional response, provided substantial improvements to the patient's perception of quality life. The association of surgery and intralesional corticosteroid was the most effective, however it would not be feasible to apply it in all corporeal lesions.
1. Schettini APM, Eiras J da C, Cunha M da GS, Tubilla LHM, Sardinha JCG. Hanseníase históide de localização restrita. An Bras Dermatol. 2008;83(5):470-2.
2. Opromolla DVA. Manifestações clínicas e reações. Noções de hansenologia. Bauru: Centro de Estudos Dr. Reynaldo Quagliato; 2000. p. 51-8.
3. Batra N, Hatwal D, Dandona S. Histiod Leprosy - How Is It Different From Lepromatous Leprosy? A Case Report. J Med Sci Clin Res. 2014;2(3):555-8.
4. Dyer RF, Enna CD. Ultrastructure of keloid: an unusual incident involving lepromatous leprosy. Int J Dermatol. 1975;14(10):743-54.
5. Sehgal VN, Aggarwal A, Srivastava G, Sharma N, Sharma S. Evolution of histoid leprosy (de novo) in lepromatous (multibacillary) leprosy. Int J Dermatol. 2005;44(7):576-8.
6. Ledon JA, Savas J, Franca K, Chacon A, Nouri K. Intralesional treatment for keloids and hypertrophic scars: a review. Dermatol Surg. 2013;39(12):1745-57.
7. Wolfram D, Tzankov A, Pülzl P, Piza-Katzer H. Hypertrophic scars and keloids--a review of their pathophysiology, risk factors, and therapeutic management. Dermatol Surg. 2009;35(2):171-81.
8. Gold MH, McGuire M, Mustoe TA, Pusic A, Sachdev M, Waibel J, et al. Updated international clinical recommendations on scar management: part 2--algorithms for scar prevention and treatment. Dermatol Surg. 2014;40(8):825-31.
9. Meaume S, Le Pillouer-Prost A, Richert B, Roseeuw D, Vadoud J. Management of scars: updated practical guidelines and use of silicones. Eur J Dermatol. 2014;24(4):435-43.
10. Rabello FB, Souza CD, Farina Júnior JA. Update on hypertrophic scar treatment. Clinics (Sao Paulo). 2014;69(8):565-73.
The present study was conducted at the Instituto Lauro de Souza Lima, Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}