


Marta Regina Machado Mascarenhas1; João Marcos Goes de Paiva1; Lais de Abreu Mutti1; Marcia Maria Vivan1; Samira Yarak2
Keloids are dermal fibroproliferative benign disorders that develop at the site of cutaneous injury, due to an imbalance of the mechanisms that control tissular repair and regeneration. The pathogenesis is not well understood, however it is postulated that an imbalance between anabolic and catabolic factors occurs in the healing process, resulting in overproduction of collagen. There are several treatment modalities, nevertheless recurrence rates are high. The objective of the present paper is to describe five cases of keloid in the ear lobe that showed a good response to a combination therapy: excisional surgery, corticosteroid injection, and pressure device.
Keywords: KELOID; AMBULATORY SURGICAL PROCEDURES; ADRENAL CORTEX HORMONES; PRESSURE
Keloid is an abnormal proliferation of cicatricial tissue formed during the healing process, usually in the location of cutaneous injuries. It does not regress spontaneously, grows beyond the original edges of the scar and should not to be mistaken with hypertrophic scars, which are elevated, do not grow beyond the original margins and can regress over time.1, 2 It occurs in a percentage that varies from 5% to 15% of scars, only in humans, at a mean onset age of between 10 and 30 years.
In general, it arises within one year after the event of a cutaneous injury and is 15 times more common in individuals with more intensely pigmented skin than in those with less pigmented skin.3 Prolonged inflammation is one of the major risk factors for the development of keloid. 4 Some regions of body are more susceptible to the formation of keloids, such as the anterior thorax, anterior surface of the neck, shoulders, arms, ears and in wounds perpendicular to the skin's tension lines. 4
The keloid's pathogenesis is poorly understood and involves alterations in the anabolic and catabolic phases of the healing process, which can be influenced by many local and genetic factors, ultimately leading to a production of collagen that is greater than its degradation. 3-5
Growth factors and cytokines are intimately involved in this process. There is an increase in transforming growth factor β (TGF-β), that regulates the proliferation of fibroblasts and collagen synthesis, promoting the differentiation of fibroblasts into myofibroblasts. Myofibroblasts present an important role in the contraction and remodeling of granulation tissue due to its ability to contract actin filaments and to increase the synthesis of collagen.
Other factors involved include the increase in mast cells, elastin, glycosaminoglycans, tumor necrosis factor α (TNF-α), interferon β (IFN-β), platelets derived growth factor (PDGF), insulin-like growth factor 1 (IGF-1) and interleukin 6 (IL-6), in addition to the decrease of the apoptosis in fibroblasts and of factors that reduce the synthesis of collagen type I, III, and possibly IV (TNF-β, IFN-α and g, and metalloproteinase 9).4, 5 There is also alteration of the immune response, with a predominance of Th2 lymphocytes that promote fibrogenesis at the expense of Th1 lymphocytes, which attenuate the fibrosis of tissues.4, 5
There are no guidelines for the treatment of keloids, and among the diverse treatment modalities, there is an effort aimed at achieving the best treatment - one that offers the lowest recurrence rate, due to the aesthetic and functional alterations as well as the impact on the patient's quality of life that these lesions cause. 5, 6
The objective of the present paper is to report five cases of keloid in the ear lobe that did not recur after being treated with a combination therapy: excisional surgery, corticosteroid injection and the use of a pressure device.
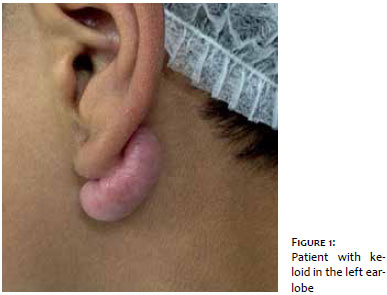
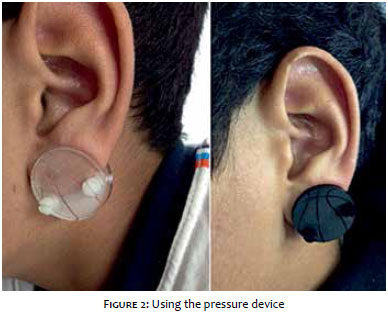
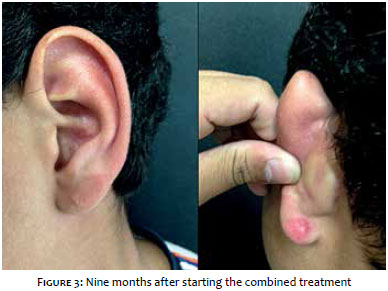
CASE 1: VJS, 14 years old, phototype III, describes the appearance of a keloid in the lobe of the left ear (Figure 1), two years before, after having the ear pierced. The partial removal of the keloid was performed 10 months before the present paper was approved for publication, with subsequent local monthly injection of 40mg/ml triamcinolone acetonide and the use of a pressure device (Delasco®,Council Bluffs, Iowa, USA) for 8 to 12 hours daily (Figure 2). Outcome nine months after the beginning of the treatment (Figure 3).
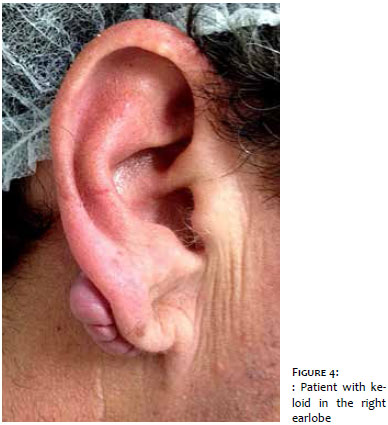
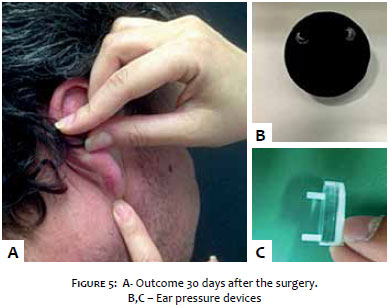
CASE 2: LPR, 46 years old, phototype III, developed keloids in the earlobes following the piercing of the ears (Figure 4). Underwent four previous surgeries and serial injections of corticosteroids without success. Three months before the present paper was approved for publication, the partial removal of the keloid was carried out in the right ear, associated with monthly injections of triamcinolone acetonide and use of pressure devices (Figure 5).
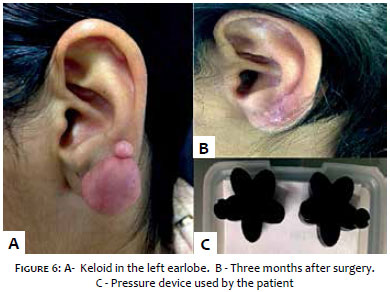
CASE 3: AGP, 21 years old, phototype V, alleges having keloids in both earlobes for six years. Has undergone two previous surgeries, with recurrence. The partial removal of the keloid was performed three months before the present paper was approved for publication. The patient is in use of pressure device and monthly triamcinolone acetonide injections (Figure 6).
CASE 4: ACSS, 40 years old, phototype V, describes the emergence of a keloid in the right ear lobe two years before the present paper was approved for publication. The patient had previously undergone six injections of corticosteroids without success. One year before the present paper was approved for publication the partial removal of the keloid was performed, associated with local injection of 40mg/ml triamcinolone acetonide and the use of a pressure device for 8 to 12 hours daily (Figure 7).
CASE 5: DC, 25 years old, phototype III, reports the onset of bilateral auricular keloids five years before. Surgery to partially remove the keloid was performed three years before. Injections of corticosteroids have been applied since then, combined with the continuous use of a pressure device, without recurrence (Figure 8).
All cases underwent intralesional excision of the keloid with an almost complete removal, leaving in place a thin portion of the affected tissue, where primary suture was performed with nylon thread 5.0. The stitches were removed ten days after, with the introduction of intralesional corticosteroid injections and the use of pressure devices.
Keloids are a therapeutic challenge, especially in individuals with less pigmented skin, for despite the lower incidence in this population group, there is greater difficulty in achieving therapeutic success. 7 Auricular keloids can affect the ear's helix, anti-helix and lobe, and are mainly associated with the use of earrings and thermal burns. An incidence of 2.5% has been verified in people who wear earrings in that region. 8
Various treatment modalities have been used to take care of keloids. Monotherapy with excisional surgery has high recurrence rates (45%-100%), and the formation of bigger keloids than the previous is common. When in combination with other methods, recurrence rates fall to 8%-50%. 1 Thus, combined treatments have proven more effective in the treatment of keloids. 9
Rathee et al. believe that in keloids located in earlobes, the excision should be intralesional (excision of the central portion of the lesion and primary closure with minimum tension) in order to reduce stimuli for collagen formation - given that the total excision promotes stimulus for further production of collagen. This results in good cosmetic outcome due to the fact that it does not alter adjacent anatomical structures. 10
The injection of corticosteroids is the therapy of choice for small and recent keloids, and is an important adjuvant treatment in larger and refractory keloids. It has primary effects on the suppression of inflammatory processes and secondary effects, such as the reduction of the synthesis of collagen and glycosaminoglycans, as well as the inhibition of growth factors. 4, 5
It is believed that the pressure devices promote hypoxia, collagen degradation and increased collagenase activity due to the reduction of the α-macroglobulins activity. 1 In addition to reducing the time of scar formation, they re-direct the collagen fibers and increase the levels of hyaluronic acid. 6 As a result, pressure earrings (ear pressure devices) were developed with the following characteristics: non-flammability, easiness of placement and removal by the patient, capability of promoting the adequate pressure, easiness of cleaning and being aesthetically acceptable. 9 There are different shapes for these devices, some of them with adaptations for the ear helix region.
Treatment recommendations with pressure earrings are not well defined, however it is postulated that the exerted pressure should be between 25-40mmHg and should be applied for 12-24 hours a day for periods ranging from months to years. 1, 6 Bran et al. report that the combination of surgery and postoperative pressure treatment leads to good response in 90-100% of cases, especially in the treatment of auricular keloids. 6 In line with the literature, 1-10 the cases reported in the present study showed good response to the combined therapy, with absence of reports of recurrence to date. However, long term monitoring is necessary for the detection of possible recurrences and early re-operation, in order to that the desired therapeutic success be achieved.
Keloids arise as a frequent complaint in dermatology practices, especially due to the impact on the quality in life caused by aesthetic changes. The authors believe that the combined treatment, with the use of aesthetically acceptable devices, is more effective, with lower recurrence rates when compared to the monotherapy, being a good therapeutic choice for the keloids in the earlobes.
1. Vivas AC, Tang JC, Maderal AD, Viera MH. Hypertrophic scars and keloids, part 1: conventional treatments. Cosmet Dermatol. 2012;25:309-16.
2. Atiyeh BS, Costagliola M, Hayek SN. Keloid or hypertrophic scar: the controversy: review of the literature. Ann Plast Surg. 2005;54(6):676-80.
3. Alhady SM, Sivanantharajah K. Keloids in various races. A review of 175 cases. Plast Reconstr Surg. 1969;44(6):564-6.
4. Bux S, Madaree A. Involvement of upper torso stress amplification, tissue compression and distortion in the pathogenesis of keloids. Med Hypotheses. 2012;78(3):356-63.
5. Gauglitz GG. Management of keloids and hypertrophic scars: current and emerging opinions. Clin Cosmet Investig Dermatol. 2013;6:103-14.
6. Bran GM, Brom J, Hormann K, Stuck BA. Auricular keloids. Combined therapy with a new pressure device. Arch Facial Plast Surg. 2012;14(1):20-26.
7. Sand M, Sand D, Boorboor P, Mann B, Altmeyer P, Hoffmann K, et al. Combination of surgical excision and custom designed silicon pressure splint therapy for keloids on the helical rim. Head Face Med. 2007;3:14.
8. Sousa RF, Chakravarty B, Sharma A, Parwaz MA, Malik A. Efficacy of triple therapy in auricular keloids. J Cutan Aesthet Surg. 2014;7(2):98-102.
9. Savion Y, Sela M, Sharon-Buller A. Pressure earrings as an adjunct to surgical removal of earlobe keloids. Dermatol Surg. 2009;35(3):490-92.
10. Rathee M, Kundu R, Tamrakar AK. Custom made pressure appliance for presurgical sustained compression of auricular keloid. Ann Med Health Sci Res.2014;4(2):147-51.
The present study was conducted at the Dermatology Department, Universidade Federal de São Paulo (Unifesp) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}