


Frederico Hassin Sanchez1; José Saulo Torres Delgado2
The reconstruction of nasal surgical defects, especially when there is total thickness bilateral simultaneous involvement of the nasal ala, tip, and dorsum, is complex. Several surgical options are described, and most authors recommend ear cartilage graft or chondro-mucous flap of the nasal septum, associated with the frontal median flap in order to lend structural rigidity to the nasal ala, preventing it from collapsing during inspiration. The authors describe an alternative reconstruction technique without the use of cartilage through the combination of hinge flaps from the nasogenian fold, associated with a frontal paramedian flap.
Keywords: MOHS SURGERY; CARCINOMA, BASAL CELL; NOSE NEOPLASMS; SURGICAL FLAPS; NASAL CARTILAGES
The incidence of skin cancer in the nose is high, with basal cell carcinoma (BCC) being the most prevalent. 1, 2
In addition to its olfactory function, the nose allows the passage of air to the upper airways, filtering and moistening the air, furthermore it has an important role in the phonation. Cosmetically, the nose is divided into subunits according to the local characteristics of each area, namely: the nasal tip, the nasal ala, the columella, the sides of the nose, the nasal dorsum and the glabella. 1, 3
Recurred tumors or of aggressive histological subtype can have great subclinical extension and affect deep structures, such as bone and cartilage, causing great functional and cosmetic damage to the patient. 4, 5
Several treatments are described for the BCC, and due to the high accuracy of the histological control of surgical margins, the Mohs micrographic surgery is the method of choice for aggressive or recurrent tumors, since it has a better chance of cure with the lower recurrence rates 4, 6 - and with the additional advantage of sparing the justatumoral healthy tissue.4, 6
Extensive infiltrative tumors can affect the cartilage of the nasal ala, causing its transfixing or full amputation, along with the nasal tip, leading to complex surgical defects. 4, 7 Surgical repair of such defects is challenging, especially due to the fact that it requires that the used technique lends sufficient structural stability to overcome the lack of alar cartilage and the collapse of the nasal ala during inspiration. 4, 7
The paramedian frontal flap, first described in India, has been used for centuries in the reconstruction of the distal third of the nose,7 while the use of ear helix or auricular concha grafts is classically described in association with the paramedian flap, 4, 7 aimed at promoting adequate support when there is total or partial amputation of the nasal ala.7 In 1902, De Quervain 8 described the use of the chondro-mucous hinged-door composite nasal septum flap for the reconstruction of the nasal lining and lateral wall. Kazanjian and Converse 9 have demonstrated the use of septal tissues for restoring the nasal lining.
Although most articles recommend the use of cartilage, the authors of the present article argue that even when extensive and full thickness nasal ala defects occur, with partial loss of the alar cartilages, the use of cartilage flaps or grafts aimed at providing structural support to the nasal ala is not always imperative.
The present article describes an option that does not use cartilage in the total reconstruction of the nasal ala, tip and dorsum, through the combination of a paramedian flap associated with a bilateral hinged-door flap, originating in the nasogenian fold.
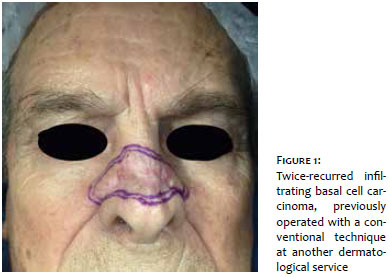
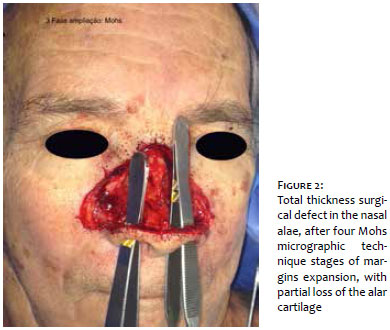
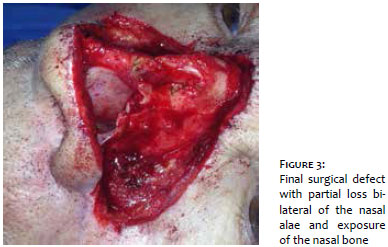
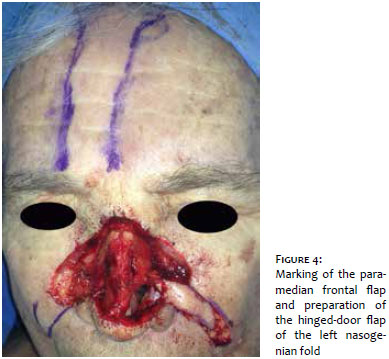
An 83 year-old male patient with infiltrating basal cell carcinoma that had recurred twice, in the nasal dorsum, was selected for Mohs micrographic surgery. The lesion measured approximately 3 x 2 cm, extending towards the lateral regions of the nose and malar bilaterally (Figure 1). Free margins were obtained after four expansion phases, with involvement and bilateral partial loss of the alar cartilages (Figure 2), and transfixion of the nasal ala and mucosa, as well as loss of the nasal dorsum and part of the nasal tip (Figures 3 and 4).
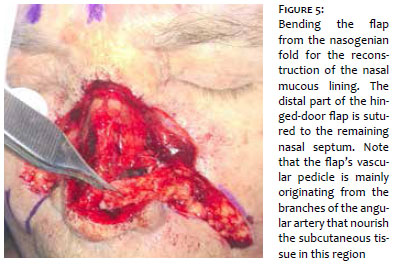
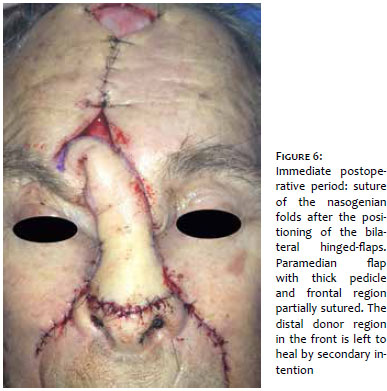
The first step is aimed at reconstructing the mucosa lining of the nasal alae through the bilateral preparation of hinged-door flaps, originating in the nasogenian folds. These flaps are drawn by measuring size of the defect to be covered, simulating the desired slope of the nasal ala with a piece of gauze. The flap is detached from the nasogenian fold, leaving a thick subcutaneous pedicle in its proximal portion to ensure the vascularization of the flap's distal portion (Figure 5). The flap's face, covered with epidermis, is folded over itself, and its distal portion is sutured to the remaining nasal septum, forming a tent, which allows the passage of air and will originate the internal part of the nasal ala (Figure 6). The donor area in the nasogenian fold is sutured primarily. The next step consists of reducing the defect of the paranasal malar region and of the lateral walls of the nose, which is done with the simple displacement of the malar region's skin and suture in the lateral nasal wall's periosteum.
The following step is aimed at constructing the paramedian flap. The defect to be covered with the flap is measured with a gauze from its base, which is located in the upper area of the medial portion of the eyebrow. The size of a flap capable of completely covering the nose's defect is estimated with the rotation of the gauze towards the frontal region. The flap - that must cover the nose - is drawn according to the shape of the surgical defect 10 and detached in three different depths in the frontal region (superficial in the distal part, near the hair line; subgaleal in the central part; and supraperiosteal in the proximal portion, 10 beside the vascular pedicle, represented by the supratrochlear artery.
After the detachment of the flap from the frontal region, it is transposed to cover the surgical wound in the area nasal, ideally with little tension and avoiding excessively bending the vascular pedicle, which would cause ischemia and distal necrosis of the flap. The attachment of the flap is initially performed in the nasal tip by means of simple suture in a way to position and guide the other fixation points. The flap's distal lateral parts are fixed on the hinged-door flaps in order to reconstruct the nasal alae. The donor area and frontal region is sutured primarily in its medial portion; the distal portion located close to the hair line is left to heal by secondary intention.
The flap is left in the position with its vascular pedicle for about three weeks, up until its autonomization. Nasal plugs made of gauze are left in place for seven days.
The flap's viability is checked after three weeks by testing the ischemia of the pedicle, pressing it with a Pean forceps, using a tourniquet or simple digital pressure. If the flap's skin remains flush, this is a sign in what the neovascularization from the receiving area is sufficient to nourish the flap and the pedicle can be sectioned.
The proximal portion of the pedicle is then returned to the original area, in the frontal region. The pedicle's central portion can be discarded along with the remaining excess tissue, with the distal portion being molded on the receiving area aimed at obtaining the best possible cosmetic outcome.
The patient progressed without complications, and the removal of the stitches took place seven days after the autonomization of the flap. The area left to heal by secondary intention (frontal region), epithelized completely in 90 days. Good aesthetic and functional results could be observed 12 months after the surgery (Figure 7).
The bilateral hinged-door flaps, with their distal portion sutured in the nasal septum, promote a proper tent effect, allowing the free passage of air through the nostrils. The layout of the tissue, forming a sandwich of skin due to the combination of the hinged-door flap with the medial frontal flap in the region of the nasal alae, sutured to the remaining tissues, promoted adequate structural rigidity, preventing its collapse during inspiration.
The combination of the hinged-door flap of the nasogenian fold with the paramedian frontal flap can be a good option for the reconstruction of multiple anatomical subunits of the distal portion of the nose, given that it provides adequate structural support, with good functional and aesthetic results, without the need for cartilage grafts.
1. Choi JH, Kim YJ, Kim H, Nam SH, Choi YW. Distribution of Basal Cell Carcinoma and Squamous Cell Carcinoma by Facial Esthetic Unit. Arch Plast Surg. 2013;40(4):387-391.
2. Davinder J. Singh, Scott P. Bartlett. Aesthetic considerations in nasal reconstruction and the role of modified nasal subunits. Plast Reconstr Surg. 2003;111(2):639-51.
3. Sanchez FH., Estefan JL, Fernandez ID. Reconstrução completa de asa nasal com retalho de Spear após cirurgia micrográfica de Mohs no tratamento de carcinoma basocelular. Surg Cosmet Dermatol 2013;5(4):35-5¬9.
4. Włodzimierz Więckiewicz, Andrzej Bieniek, Mieszko Więckiewicz, Lukasz Sroczyk. Interdisciplinary treatment of BCC located on the nose - review of literature. Adv Clin Exp Med. 2013;22(2):289-93.
5. Charlotte M. Clark, Megan Furniss, Julian M. Mackay-WigganBasal cell carcinoma: an evidence-based treatment update. Charlte M. Clark, Megan Furniss, Julian M. Mackay-Wiggan. Am J Clin Dermatol. 2014;15(3):197-216.
6. Fletcher KC Jr, Shonka DC Jr, Russell MA, Park SS. Defects of the nasal internal lining: etiology and repair. Arch Facial Plast Surg. 2005;7(3):189-94.
7. De Quervain F. Uber partielle seitliche Rhino- plastik. Zentralbl. Chir.1902;29:297.
8. Kazanjian V H., and Converse, J. M. The Surgical Treatment of Facial Injuries. Baltimore: Willians and Wilkins; 1949. p. 349-53.
9. Cerci FB, Nguyen TH. Retalho paramediano frontal na reconstrução de defeitos nasais complexos após cirurgia micrográfica de Mohs. Surg Cosmet Dermatol 2014;6(1):17¬-24.
10. Salmon PJ., Mortimer NJ, Hill SE. Muscular Hinge Flaps: Utility and Technique in Facial Reconstructive Surgery. Dermatol Surg. 2010;36(2):227-34.
The present study was conducted at the Centro de Cirurgia Micrográfica do Rio de Janeiro, Policlínica Ronaldo Gazolla - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}