


Fernanda Berti Rocha Mendes1; Raquel de Paula Ramos Castro1; Mariana Petaccia de Macedo2; Clovis Antonio Lopes Pinto2; João Pedreira Duprat Neto3; Gisele Gargantini Rezze1
Recurring nevus or pseudomelanoma is a benign melanocytic lesion that appears in the same location after an incomplete surgical removal of nevi. These pigmented melanocytic lesions can in some cases be a diagnostic challenge when examined through dermoscopy, especially if there is a clinical history of growth or recurrence of the lesion, as happens with the recurrent nevus phenomenon. Confocal reflectance microscopy is an in vivo non-invasive imaging technique with high histomorphological resolution of the skin that can be used to differentiate between benign and malignant lesions, increasing the in vivo diagnostic accuracy. Nonetheless, in some cases only the histological and immunohistochemical examinations of the complete lesion can clarify the diagnosis.
Keywords: CARCINOMA, BASAL CELL; EPIDEMIOLOGY; SKIN NEOPLASMS; PATHOLOGY; DERMATOLOGY
Recurrent nevus (RN) is a benign melanocytic lesion, which appears in the same skin topography after an incomplete surgical removal, such as shave biopsy, incisional biopsy, either ablative or non ablative laser (erbium, Q-switched), dermabrasion, electrocautery, chemosurgery, excision surgery with compromised margins or even local trauma. 1 In 1975, Korneg and Ackerman named recurrent nevi by pseudomelanoma, due to histological and clinical features mimicking superficial spreading melanoma. 2 These pigmented melanocytic lesions, can in some cases become a diagnostic challenge using dermoscopy, especially if there is a clinical history of growth and recurrence of the lesion, as it occurs in the RN phenomenon. Reflectance confocal microscopy (RCM), a noninvasive in vivo technique for obtaining high-resolution histomorphological images of the skin, is useful to differentiate benign from malignant lesions, improving the accuracy of in vivo diagnosis. 3-7
A 49-year-old white male, without personal or family history of melanoma, presented with a pigmented melanocytic lesion in his left arm. It had been partially removed through surgery eight years before at another service, without histological examination, and was recently growing and becoming darker. The patient presented history of clear cell kidney carcinoma.
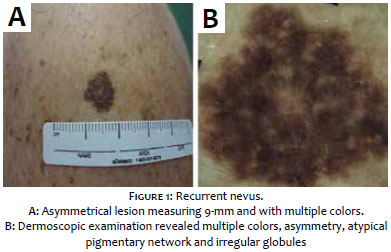
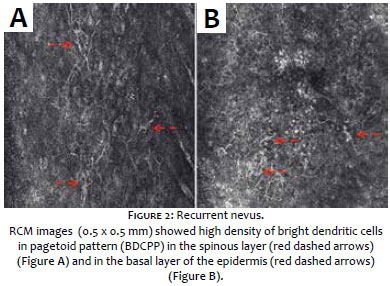
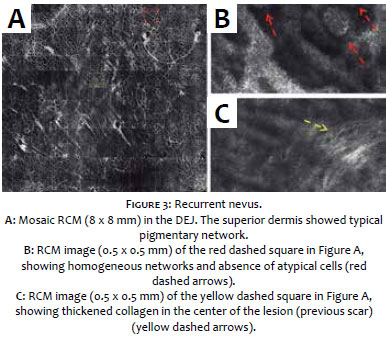
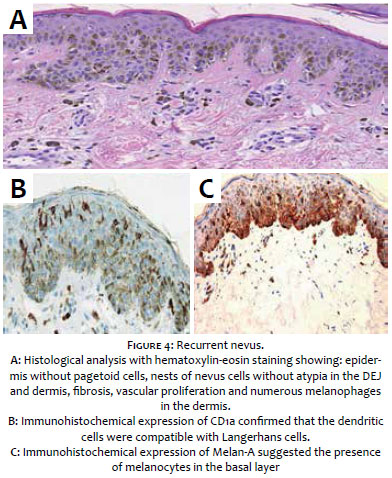
Dermoscopic examinations revealed multiple colors (dark brown, light brown and gray), asymmetry, atypical pigmentary network, irregular globules and blotch areas in the lesion's extremities (Figure1). The in vivo reflectance confocal microscopy (RCM) was performed due to the diagnostic hypothesis of melanoma. The RCM showed high density of bright dendritic cells in pagetoid pattern (BDCPP), possibly corresponding to atypical melanocytes or Langerhans cells in the epidermis (Figure 2), with a dendritic stellate morphology, from the basal layer up until the upper spinous layer of the epidermis. A typical reticular pattern, homogeneous networks and absence of atypical cells were observed in the dermal-epidermal junction (DEJ) and superior dermis, with thickened collagen in the lesion's center (previous scar) (Figure 3). Surgical resection with 2mm margin was performed and the histological analysis revealed no atypical cells in the epidermis, nests of nevus cells without atypia in the DEJ and dermis, fibrosis, vascular proliferation and numerous melanophages in the dermis (Figure 4). Immunohistochemistry was performed due to the presence of dendritic cells in the epidermis (seen in the RCM). CD1a positivity confirmed the presence of a large number of Langerhans cells scattered in the epidermis, while Melan-A showed the presence of melanocytes confined in the basal layer (Figure 5).
Recurrent nevus is a benign melanocytic lesion, mostly predominant in young female adults, that occurs within 6 weeks to 6 months after an incomplete surgical removal in the same skin topography. It usually presents macular pigmentation perpendicular to the scar, positioned from the center to the periphery, being linear or homogeneous, with striae distributed in the shape of a "leaf", containing globules and networks. On the other hand, recurrent melanomas seem to have pigmentation beyond the scar's area, towards the normal skin, without continuity, being asymmetrical and having more than two colors.8 Botella-Estrada et al. described a sensitivity and a specificity of 72% and 90%, respectively, for RN using dermoscopy.
Although the in vivo RCM is very useful to identify malignant melanocytic lesions, differentiating intraepidermal Langerhans cell (LC) from melanocytes is still a challenge given that both are bright dendritic cells spreading in a pagetoid pattern.9 Pelacani et al. described the pagetoid spread of melanocytes as a major criteria for melanoma diagnosis,10 nevertheless in some cases with high density of LC in the stratum spinosum of the epidermis, this lesion can be misdiagnosed as a melanoma in a false-positive in RCM, as it occurred in the present case.
Up to 2% of LC are expected to be found in the epidermis of normal skin,4 with this figure varying in accordance with the body topography. 9, 11 In the present RCM case report, the LC's morphology was observed as pleomorphic, with some thick and long dendrites spreading into epidermis, from the basal layer towards the superior epidermis. This fact contrasts with the literature described before regarding the differentiation of LC from melanocytes in pagetoid pattern melanomas, in which thin and shorter dendrites would be expected, in addition to rare cells distributed across the lesion. 9 Hashemi et al concluded the most important characteristic in RCM used to distinguish melanomas from nevi is the density of the BDCPP, which is more expressive in the first. However in the present case report, there was a high density of BDCPP in a benign lesion. An additional diagnostic challenge in the present case was the fact that the patient did not remember he had undergone a previous incisional biopsy, which is not uncommon in the clinical dermatologic practice.
The hematoxylin-eosin based histology suggested the presence of compound nevi, which is not compatible with the features seen in the epidermal layer through RCM. Therefore an immunohistochemical study for CD1a was necessary. It exhibited a high density of LC in the epidermis from the basal layer up until the superior region of the spinous layer, clarifying the RCM findings.
These pigmented lesions can clinically be a diagnostic challenge in the differentiation from melanomas, and RCM can increase the noninvasive diagnostic accuracy, particularly due to the presence of BDCPP. However, if there is lack of other RCM characteristics of cutaneous melanoma, as the atypical cells in the DEJ, the existence of BDCPP possibly corresponds to Langerhans cells, as evidenced by immunohistochemistry.
1. Fox JC, Reed JA, Shea CR. The recurrent nevus phenomenon - A history of challenge, controversy, and discovery. Arch Pathol Lab Med. 2011;135(7):842-6.
2. Kornberg R, Ackerman AB. Pseudomelanoma: recurrent melanocytic nevus following partial surgical removal. Arch Dermatol. 1975;111(12):1588-90.
3. Oliveira A, Arzberger E, Massone C, Fink-Puches R, Zalaudek I, Hofmann-Wellenhof R. Dermoscopy, reflectance confocal microscopy and immunohistochemical analysis in melanocytic lesions with Meyerson's Phenomenon. Dermatology. 2014;229(4):297-305.
4. Cinotti E, Labeille B, Perrot JL, Douchet C, Cambazard F. Cells of Langerhans cell histiocytosis and epidermal Langerhans cells differ under reflectance confocal microscopy: first observation. Skin Res Technol. 2014;20(3):385-7.
5. Longo C, Moscarella E, Pepe P, Cesinaro AM, Casari A, Manfredini M, et al. Confocal microscopy of recurrent naevi and recurrent melanomas: a retrospective morphological study. Br J Dermatol. 2011;165(1):61-8.
6. Larre Borges A, Zalaudek I, Longo C, Dufrechou L, Argenziano G, Lallas A, et al. Melanocytic nevi with special features: clinical-dermoscopic and reflectance confocal microscopic-findings. J Eur Acad Dermatol Venereol. 2014;28(7):833-45.
7. Maio P, Antunes J, Pacheco D, Almeida LS, Marques MS. Nevos recorrentes - uma revisão de 5 anos. Revista SPDV. 2012;70(2):183-7.
8. Botella-Estrada R, Nagore E, Sopena J, Cremades A, Alfaro A, Sanmartín O, et al. Clinical, dermoscopy and histological correlation study of melanotic pigmentations in excision scars of melanocytic tumours. Br J Dermatol. 2006;154(3):478-84.
9. Hashemi P, Pulitzer MP, Scope A, Kovalyshyn I, Halpern AC, Marghoob AA. Langerhans cells and melanocytes share similar morphologic features under in vivo reflectance confocal microscopy: a challenge for melanoma diagnosis. J Am Acad Dermatol. 2012;66(3):452-62.
10. Pellacani G, Cesinaro AM, Seidenari S. Reflectance-mode confocal microscopy for the in vivo characterization of pagetoid melanocytosis in melanomas and nevi. J Invest Dermatol. 2005;125(3):532-7.
11. Roediger B, Ng LG, Smith AL, Fazekas de St Groth B, Weninger W. Visualizing dendritic cell migration within the skin. Histochem Cell Biol. 2008;130(6):1131-46.
The present study was conducted at AC Camargo Câncer Center - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}