


Maria Helena Mazzi Freire Nigro1; Leticia Stella Gardini Brandão2; Ana Paula Cota Pinto Coelho3; Leticia Marra da Motta1; Ivander Bastazini Júnior4
Introduction: Basal cell carcinoma is the most common skin cancer and corresponds to 70-80% of all malignant neoplasms of the skin. It is emerging as a global public health problem, with incidences of the condition increasing in all countries. Objective: To evaluate the epidemiological profile and characteristics of patients diagnosed with basal cell carcinoma in the previous four years in a reference hospital. Methods: A cross-sectional descriptive study was carried out at a dermatology reference center in the city of Bauru, São Paulo State, Brazil. Patients diagnosed with basal cell carcinoma, confirmed by histological examination from January 2010 to December 2013 were included in the study. The variables analyzed descriptively were: age at diagnosis, gender, city of origin, site of lesion, and race. Results: A higher incidence of basal cell carcinoma was observed in Caucasian women older than 60 years, with the malar and nasal regions arising as the usual locations. Conclusions: There is an increased incidence of basal cell carcinoma in young people, however the most affected population is still the elderly Caucasian population. The most common area for the cancer is the face, particularly the upper two thirds. The incidence of this cancer in younger populations is worrying, with the dermatologist having an important role in the prevention and early treatment.
Keywords: CARCINOMA, BASAL CELL; EPIDEMIOLOGY; SKIN NEOPLASMS; PATHOLOGY; DERMATOLOGY
Basal cell carcinoma (BCC) is a cutaneous neoplasm that originates from pluripotent immature basal epithelial cells that lost their normal differentiation and keratinization capacity, as well as of those of the skin adnexa.1 It is the most common skin cancer in the world, and in Brazil it corresponds to 70-80% of the malignant cutaneous neoplasms.2: 6-8 It affects mainly white males above 40 years of age with history of chronic exposure to the sun. Its preferred location is the face, especially the two upper thirds. Exposure to ultraviolet radiation is the main environmental risk factor associated with its genesis. More recently, BCC has demonstrated alterations in its presentation, such as involvement of unexposed areas and tendency to higher incidence in females.3,4,6 The cumulative risk of BCC in the white population is more than 30%, and its incidence has been increasing in all countries, configuring a growing public health problem.2 The BCC is a slow-growing, locally aggressive neoplasia, however it is rarely able to generate metastases.3, 6 The most frequent clinical subtype is the nodular-ulcerative, which occurs more frequently in areas exposed to the sunlight, followed by the superficial subtype, which is more prevalent in the trunk region. The diagnosis is clinical and confirmed by histology, and surgery remains the therapy of choice.1,5 The present study was aimed at evaluating the epidemiological profile and characteristics of patients with BCC seen from 2010 to 2013 at the Istituto Lauro de Souza Lima, a tertiary referral hospital in dermatology, located in the city of Bauru (SP), Brazil, correlating the findings with data already published in the literature.
A transversal descriptive study was carried out based on a research performed on the database of a reference service in dermatology, including patients bearers of BCC confirmed by histological examination, between January 2010 and December 2013. The variables analyzed - only descriptively - were: age at diagnosis, gender, city of origin, location of lesion and ethnicity.
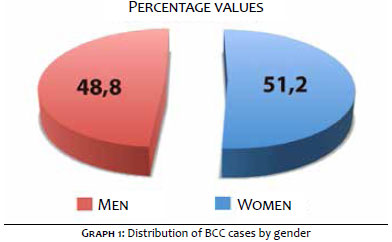
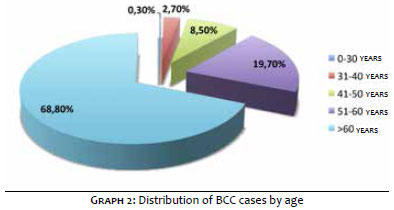
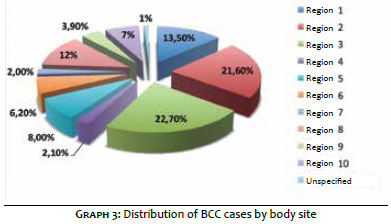
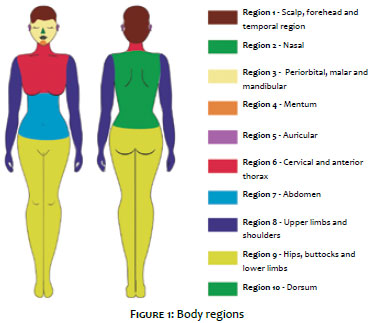
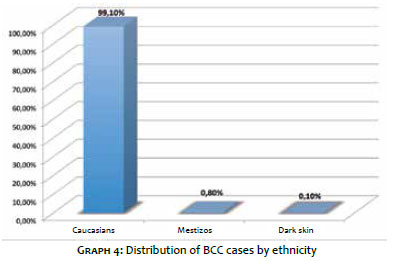
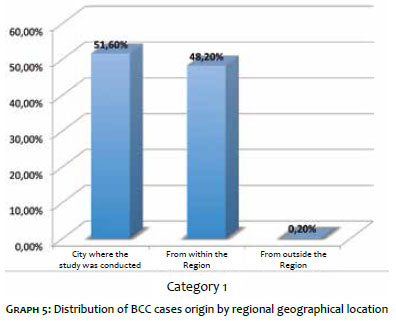
Between 1st January 2010 and 31st December 2013 1,968 reports with BCC diagnosis were identified for a total of 1,150 patients, with an average of 1.7 lesion per patient. The maximum number of lesions with diagnosis of BCC in the same occasion was 7, and the maximum number of BCCs in the same patient during the four years period was 13. Of the patients with BCC, 51.2% were female and 48.8% were male (Graph 1). The age ranged from 21 to 97 years, with patients grouping into five categories: up to 30 years (0.3%), 31-40 years (2.7%), 41-50 years (8.5%), 51-60 years (19.7%) and over 60 years - the latter with an absolute majority of cases (68.8%) (Graph 2). The location of the lesion was marked according with ten anatomical regions: 1) forehead, temporal and scalp (13.5%), 2) nose (21.6%), 3) malar, maxillary, mandibular and periorbital (22.7%), 4) mentum (2.1%), 5) auricular, pre-auricular and retroauricular (8%), 6) cervical region and anterior thorax (6.2%), 7) abdomen (2%), 8) shoulders and upper limbs (12.0%), 9) hip, buttocks and lower limbs (3.9%), 10) dorsum (7.0%), and 11) unidentified location (1.0%) (Graph 3 and Figure 1). Patients were also grouped in Caucasians (99.1%), mestizos, mulattos and yellow (0.8%), and dark skin individuals (0.1%) (Graph 4). It has also been found that 51.6% of the patients analyzed were originary from the city where the study was carried out, and 48.2% from municipalities in the city of Bauru (SP) region, for the hospital functions as a reference center to 67 cities, with only 0.2% of cases being originated outside the region (Graph 5).
The high morbidity caused by BCC in advanced stages is a public health problem. Prevention and early diagnosis, in addition to the knowledge about risk factors are crucial for the reduction in the morbidity. The lack in information on the epidemiology of BCC in the Brazilian population justifies this study. The findings linked to gender suggest absence of significant difference between the percentage of affected men and women. In the present study, a higher incidence of BCC in women as compared to men was observed - a finding that differs from much of the published literature - 5 however more recent studies have shown that change in the pattern of occurrence. 3, 4, 6, 8, 9 It is possible to notice an increase in the incidence of BCC in younger patients, which can be partly explained by the tanned skin culture and more time available for leisure. Nevertheless, patients with over 60 years of age remain the most affected group by the neoplasm, in line with the remaining of the reviewed literature. There was almost absolute predominance of Caucasians, as described in the literature. 1-9 However, this result can be questioned, since the ethnicity classification is subjective and defined by the patient him or herself when answering the admission questionnaire. Regarding the location of the lesion, it was possible to observe a higher incidence of BCC on areas exposed to the sun, predominantly in the face, with emphasis on the malar region and the nose region. Covered areas, such as legs and trunk, showed very little incidence. It was not possible to group the lesions according to their histological type, since the service's pathology department does not make that differentiation among the neoplasms found.
The present study is aligned with most of the current literature, which has been showing a progressive increase in the involvement of women and young patients. 6 It also confirms that the Caucasian population is the most affected group by this cancer type and that exposed areas are at increased risk of developing lesions 1-9. The increased incidence of this neoplasm in the younger population is alarming. It is therefore important that this population be educated about the fact that the main causal factor of the neoplasm is the frequent and cumulative exposure to the sun, through campaigns focusing on photoprotection and guidance during dermatologic consultations.
1. Almeida ACC, Yamashita T, Conte B, Mattos AC, Veríssimo RP, Ferreira MCF. Frequência do carcinoma basocelular na população menor de 50 anos: estudo do serviço e revisão de literatura. An Bras Dermatol. 2009;84(6):692-4.
2. Schmitt JV, Chinem VP, Marques MEA, Miot HA. Aumento da incidência de carcinoma basocelular em hospital universitario: 1999 a 2009. An Bras Dermatol. 2011;86(2):375-7.
3. Mantese SAO, Berbert ALCV, Gomides MDA, Rocha A. Carcinoma basocelular - Análise de 300 casos observados em Uberlândia - MG. An Bras Dermatol. 2006;81(2):136-42.
4. Lascano AR, Kuznitzky R, Garay I, Ducasse C, Albertini R. Factores de riesgo para carcinoma basocelular- Estudio de casos-controles em Cordoba. Medicina (B. Aires). 2005;65(6):495-500.
5. Ferreira FR, Pevide BC, Rodrigues RF, Nascimento LFC, Alvarenga Lira ML. Differences in age and topographic distribution of the different histological subtypes of basal cell carcinoma, Taubaté (SP), Brazil. An Bras Dermatol. 2013;88(5):726-30.
6. Miot HA, Chinem VP. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
7. Bariani RL, Nahas FX, Barbosa MVJ, Farah AB, Ferreira LM. Basal cell carcinoma: an updated epidemiological and therapeutically profile of an urban population. Acta Cir Bras. 2006;21(2):66-73.
8. Souza CFD, Thomé EP, Menegotto PF, Schmitt JV, Shibue JRT, Tarlé RG. Topografia do carcinoma basocelular e suas correlações com o gênero, a idade e o padrão histológico: um estudo retrospectivo de 1.042 lesões. An Bras Dermatol. 2011;86(2):272-7.
9. Peres LP, Fiorentin JZ, Baptista TS, Fuzina DG, Blanco LFO. Clinical and histopathological profile of basal cell carcinoma in a population from Criciuma, Santa Catarina, Brazil. An Bras Dermatol. 2012;87(4):657-9.
The present study was conducted at the Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}