


Camila Araujo Scharf Pinto1; Manuela Ferrasso Zuchi Delfes2; Larissa Montanheiro dos Reis2; Luiz Eduardo Garbers3; Paola Cristina Vieira da Rosa Passos4; Deborah Skusa de Torre5
Introduction: Melasma is a common acquired hypermelanosis of difficult treatment due to the fact that it is a refractory and recurrent condition. Pycnogenol is a powerful antioxidant that can be effective in the treatment of melasma owing to its protective action against ultraviolet radiation. Objectives: To evaluate the effectiveness of 100 mg/day pycnogenol in the treatment of melasma. Methods: Prospective, randomized, interventional study carried out with 31 patients. The selected participants made use of 100 mg / day pycnogenol and sunscreen for 90 days. They were evaluated regarding the extent of melasma (MASI) and quality of life (MELASQol). Results: Efficacy results showed a significant reduction (p <0.05) in the scores for both scales (MASI and MELASQol). According to the participants' self-evaluation, 94.4% of them showed clinical improvement. Conclusion: 50 mg pycnogenol was shown to be effective in the treatment of melasma after use of 2 tablets / day for 90 days. The results for the MASI and MELASQoL (Melasma Quality of Life Scale) scores were statistically significant. Furthermore, the product was proven to be safe due to the low incidence of side effects.
Keywords: MELANOSIS; CHEMOPREVENTION; ADJUVANTS, PHARMACEUTIC
Melasma is a common, symmetrical acquired hypermelanosis characterized by brownish, macules, with irregular contours and clear limits, in photo-exposed areas, especially the face, forehead, temples and, more rarely, in the nose, eyelids, mentum and upper limbs. 1-3 It affects both genders, with a higher incidence in women, especially during pregnancy. It occurs in all races, particularly in individuals with intermediate skin phototypes living in areas with high levels of ultraviolet radiation (UV).2
Although its pathogenesis is not entirely known, multiple factors are involved, especially the hormonal influence associated with pregnancy, oral contraceptives, hormone replacement therapy, ultraviolet A and B radiations, genetic predisposition, phototoxic drugs, anticonvulsants and thyroid dysfunction. 3-5
There is no consensus about the clinic classification of melasma. There are two recognized main patterns of facial melasma: centrofacial (which affects the central region central of the forehead, and the buccal, labial, supralabial and mentonian regions) and malar (which affects the zygomatic regions). Some authors add a third, less frequent, pattern: the mandibular pattern.4-6
The current treatment of melasma can be divided into two categories: topical and oral 5, 7, 8 Overall, both the topical and the oral treatments remain a challenge due to the refractory and recurrent character of this condition. The goal of the treatment is to reduce the synthesis of melanin, inhibiting the formation of melanosomes and promote its degradation. Regardless of the depigmenting agent used, broad-spectrum photoprotection is essential to prevent the formation of new melanin and to reduce the oxidation of the preformed melanin. 3, 8-10
Pycnogenol is an extract from the bark of French pine (Pinus pinaster), already known as potent antioxidant. In vitro studies have shown that this antioxidant is more potent than vitamins E and C. In addition, it recycles vitamin C, regenerates vitamin E and increases the endogenous enzymatic antioxidant system. Due to the fact it has a protective action against ultraviolet radiation, its efficacy in melasma has been studied. 5-7
To evaluate the effectiveness of 100 mg/day of pycnogenol in the treatment of melasma.
A prospective, randomized, interventional study was carried out after the approval of the Research Ethics Committee (CAEE 21845213.4.0000.0103) and the signing of a Free and Informed Term of Consent by the voluntary participants.
The participants were selected at the Dermatology Ambulatory of the Hospital Universitário Evangélico de Curitiba from October 2013 to December 2013. The selection criteria were: adult patients diagnosed with melasma, belonging to the age group 18 to 75 years old, female, all skin phototypes according the Fitzpatrick classification, volunteers and capable of understanding the study's objective, who were not breastfeeding or pregnant.
Participants who used diverse treatments for melasma (topical or oral) in the previous three months were excluded.
The restrictions imposed on participants were: not to use any whitening cosmetic in the face during the study, not to use medications without telling the researcher physician, not to get exposed to the sunlight or ultraviolet lamps without the use of sunscreen, and not to use photosensitizing drugs during the study.
At the beginning of the study, the participants were assessed for skin phototype (according to the Fitzpatrick classification), and for melasma (using of the MelasQoL questionnaire - Melasma Quality of Life Scale, and the Area and Melasma Severity Index - Masi). In addition, standardized photographs of the participants were taken.
The selected participants used 50mg pycnogenol (Flebon®, Farmoquímica, Rio de Janeiro, Brazil), with two concomitant tablets being administered daily, for 90 days. In addition, sunscreen (Actsun® SPF 45, Farmoquímica, Rio in Janeiro, Brazil) should be used daily, with reapplications whenever necessary. Both products were provided to the participants free of charge.
A new evaluation was performed after that period using the MelasQoL and Masi, and the standardized photographs, in addition to the perceived efficacy evaluation carried out by the participants. The latter was performed considering the following ratings: worsened, unchanged, improved (35-50%), improved markedly (50-75%). The existence of undesirable side effects was also evaluated.
The main variables representing the study's outcome were the differences in the evaluation results in the experimental time 1 and experimental time 2. Quantitative variables were represented by mean values and standard deviations or medians and quartiles (1st and 3rd), when normality was not evidenced by the Shapiro-Wilk test. The comparison between the two experimental times was performed by the Student t test or Mann-Whitney test when indicated. Qualitative variables were denoted by their percentage and compared by the chi-square test or coefficient Tau C Kendall, when there were ordinal characteristics. Two-tailed p values <0.05 were considered significant. The data were tabulated in MS Excel 2003® and analyzed using the SPSS 19 software.
Sample size
Thirty-one participants who attended the Dermatology Ambulatory of the Hospital Universitário Evangélico de Curitiba between October and December 2013 were selected.
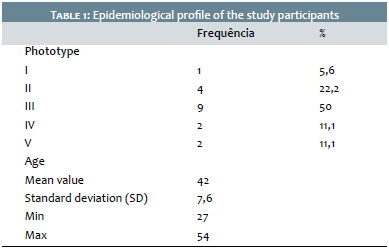
Thirty-one participants were included in the study and 18 completed it. Fifty percent of the participants evaluated had skin phototype III. The mean age was 42 years, as can be seen in Table 1.
Seven participants had comorbidities prior to the beginning of the treatment, in special: hypothyroidism, bronchitis, dyslipidemia, rheumatoid arthritis, depression and fibromyalgia.
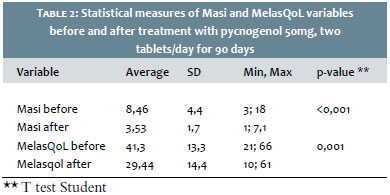
Efficacy analysis results showed a significant reduction (p <0.05) in scores for both scales - Masi and MelasQoL - as shown in Table 2. Assessing the Mai scores, it is possible to notice that the average difference before and after the treatment was of approximately 5 points (max = 7.1, min = 1.0) after the treatment. Regarding the MelasQoL scale the average difference was roughly 12 points (max = 61, min = 10) after the treatment.
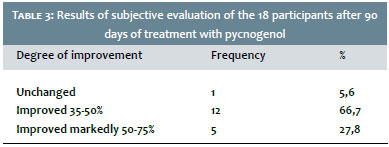
According to the evaluation perceived by the participants, 94.4% had clinical improvement as is shown in Table 3. This outcome was recorded and corroborated by the photographic assessment before and 90 days after the treatment, as illustrated in Figures 1 and 2.
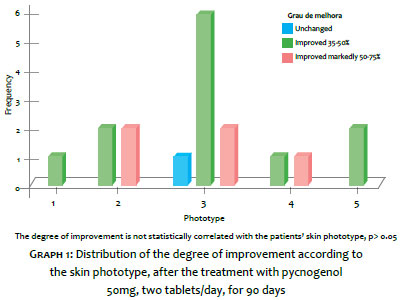
In order to verify whether there is any association between the participants' degree of improvement and skin phototype, the correlation between these two variables was assessed and proven statistically inexistent, as shown in Graph 1.
Few adverse events, such as polyuria (increased diuresis) and lower limb edema, were observed. The latter occurred in a participant who had combined the use of hormone replacement in the week before, invalidating a possible association of this event with the use of pycnogenol.
Melasma is an extremely common condition in the Dermatologic practice however it is still quite refractory to available therapies. It is known that most of the patients present satisfactory response to the use of topical treatments; nevertheless pycnogenol comes as a therapeutic option for those who maintain absence of response to multiple therapies and those aiming at maintaining the response.
Pycnogenol has the ability to inhibit the tyrosine kinase and has been demonstrating action on the regulation the biosynthesis of melanin. In vitro studies 11 have shown its ability in suppressing superoxides, oxide nitric and the radical hydroxyl, thus expressing significant antioxidant and antimelanogenic properties.
The mechanism of action of pycnogenol was studied by Cho et al.,12 who showed its inhibitory action of the gene expression of proinflammatory cytokines, based on the cultures of RAW264 cells 7 for interleukin-1 (IL-1) and Jurkat E6 cells 1 for interleukin-2 (IL-2). Pycnogenol showed significant activity against types of peroxides that generated varieties of reactive oxygen in the cells RAW264. 7 In addition, ELISA, immunoblotting and polymerase reaction (RT-PCR) studies indicated that IL-1 levels were reduced in cells that were pretreated with pycnogenol.
Other studies13, 14 have also shown that the expression of IL-1, of the factor nuclear B (NF-KB) and of the activator of the protein 1 (AP-1), were also blocked by pycnogenol, demonstrating a broad spectrum of anti-inflammatory action of the substance. Canali et al. 15 also observed action of pycnogenol on the arachidonic acid's route when providing 150mg/day for five days to volunteers aged between 35-50 years, with subsequent blood test of patients. This study allowed concluding that the anti-inflammatory action of pycnogenol was due to the reduced gene expression of COX-2, decreasing the biosynthesis of leukotrienes.
Several authors16,17 have shown interest in antioxidants, such as vitamin C and E, as well as in the very French pine extract (FPE), which repeatedly show positive results in the management of rhytids and hyperpigmentation.
In two different articles, Berson18 and Bordan Allemann19 summarized the antioxidants of natural origin, which, when applied topically, can restore the the skin's antioxidant ability. Due to the proven FPE's antioxidant capacity, it can be included in the management of certain cutaneous pathologies.
In another study conducted by Ni et al.5 with 30 women, the efficacy and safety of using pycnogenol was evaluated. Seventy-five mg per day of the product were administered for 30 days. According to the results, the participants showed a decrease in the melasma's area as well as in the pigmentary intensity after the treatment. No adverse event was reported. Pycnogenol was safe and effective for the treatment of melasma.
A study by Campos20 evaluated the efficacy and safety of the daily use of 100 mg of pycnogenol for two months in 29 women with melasma. The product was effective in 88.8% of participants, with absence of adverse event cases.
Pycnogenol 50 mg has proven effective in the treatment of melasma after the use two tablets per day for 90 days. The Masi and MelasQoL scores' results were statistically significant. Moreover, the product proved to be safe due to the low incidence of side effects.
1. Grimes PE. Melasma. Etiologic and therapeutic considerations. Arch Dermatol. 1995;131(12):1453-7.
2. Steiner Denise, Feola Camila, Bialeski Nediana, Morais e Silva Fernanda. Tratamento do melasma: revisão sistemática. Surg Cosmet Dermatol. 2009;1(2):87-94.
3. Moreira AM, Bravo BSF, Amorim AGF, Luiz RR, Issa M. Estudo duplo cego comparativo entre hidroquinona e extrato de uva-ursina no tratamento do melasma. Surg Cosmet Dermatol. 2010;2(2)99-104.
4. Miot Luciane Donid, Miot Helio Amante, Silva Marcia Guimaraes, Marques Mariangela Esther.Fisiopatologia do melasma. An Bras Dermatol. 2009;84(6):623-35.
5. Ni Z, Mu Y, Gulati O. Treatment of Melasma with Pycnogenol®. Phytother Res. 2002;16(6):567-71.
6. Gupta AK1, Gover MD, Nouri K, Taylor S. The treatment of melasma: A review of clinical trials. J Am Acad Dermatol. 2006;55(6):1048-65
7. Tamler Carla, Fonseca Rosa Maria Rabello, Burnier Francisco, Pereira Carlos, Barcauí Carlos Baptista. Classificação do melasma pela dermatoscopia: estudo comparativo com lâmpada de Wood. Surg Cosmet Dermatol. 2009;1(3):115-9.
8. Manela-Azulay M, Borges J. Estudo-piloto: tratamento de melasma com laser de Erbium fracionado não ablativo (1.540nm). Surg Cosmet Dermatol. 2011;3(4):313-8.
9. Costa A, Arruda LH, Pereira E, Pereira M, Santos FB, Fávaro R. Estudo clínico para a avaliação das propriedades clareadoras da associação de ácido kójico, arbutin, sepiwhite® e achro max y l® na abordagem do melasma, comparada à hidroquinona 2% e 4%. Surg Cosmet Dermato. 2011;3(4):22-30.
10. Hammerschmidt M, Mattos SML, Suzuki HS, Freitas CFNP, Mukai MM. Avaliação dos métodos de classificação do melasma de acordo com a resposta ao tratamento. Surg Cosmet Dermatol 2012;4(2):155-8.
11. Kim YJ, Kang KS, Yokozawa T. The anti-melanogenic effect of pycnogenol by its anti-oxidative actions. Food Chem Toxicol. 2008;46(7):2466- 2471.
12. Cho KJ, Yun CH, Packer L, Chung AS. Inhibition mechanism of bioflavonoids extracted from the bark of Pinus maritime on the expression of proinflammatory cytokines. Ann N Y Acad Sci. 2001;928:141-56.
13. Tanja Grimm, Zuzana Chovanová, Jana Muchová, Katarína Sumegová, Anna Liptáková, Zdeňka Ďuračková, et al. Inhibition of NF-B activation and MMP-9 secretion by plasma of human volunteers after ingestion of maritime pine bark extract (pycnogenol). J Inflamm (Lond). 2006;3:1.
14. Schafer A, Chovanova Z, Muchova J, Sumegova K, Liiptakova A, Durackova , et al. Inhibition of COX-1 and COX-2 activity by plasma of human volunteers after ingestion of French maritime Pine bark extract (Pycnogenol). Biomedicine & Pharmacotherapy. 2005;60:5-9.
15. Canali R, Comitato R, Schonlau F, Virgili F. The anti-inflammatory pharma- cology of pycnogenol in humans involves COX-2 and 5-LOX m RNA expression in leukocytes. Int Immunopharmacol. 2009;9(10):1145-9.
16. Chang M, Park S, Kwak TJ, Park HK, Lee CK, Lee HS, et al. Effects of the mixture of vitamin C, vitamin E, pycnogenol and evening prim- rose oil on the UV-induced pigmentation and wrinkles reduction in human skin. Korean Journal of Nutrition. 2009;42(6):516-22.
17. Cho HS1, Lee MH, Lee JW, No KO, Park SK, Lee HS, et al. Anti-wrinkling effects of the mixture of vitamin C, vitamin E, pycnogenol and evening primrose oil, and molecular mechanisms on hairless mouse skin caused by chronic ultraviolet B irradiation. Photodermatol Photoimmunol Photomed. 2007;23(5):155-62.
18. Berson DS. Natural antioxidants. J Drugs Dermatol. 2008;7(1):7-12.
19. 19. Allemann B, Bauman L. Antioxidant used in skin formulations. Skin Therapy Letter. 2008;13(7):5-8.
20. Campos, V. Oral administration of pycnogenol associated with sunscreen improve clinical symptoms of melasma. J Am Acad Dermatol. 2014;70(5):AB19.
The present study was conducted at the Hospital Evangélico de Curitiba - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}