


Ariene Murari Soares de Pinho1; Isis Sousa Oliveira Pereira2; Marina Emiko Yagima Odo3; Lilian Piñeiro Marcolin Eça4
Introduction: The dermis is mainly composed of the extracellular matrix and fibroblasts that produce collagen types I and III, and elastic fibers. Objective: To verify through a prospective, comparative controlled clinical study whether there is an increase in the production of collagen fibers in healthy human skin after the injection of autologous fibroblasts in the dermis. Methods: Two skin fragments were collected from the right retro-auricular region of four women aged between 25 and 60 years. In one of the fragments, histology was carried out with Hematoxylin-Eosin and Picrosirius to qualify and quantify the collagen fibers (Control Group). A second fragment underwent enzymatic digestion in the laboratory aimed at extracting and culturing fibroblasts. After satisfactory growth (1 x 107 cells / ml) the cultured fibroblasts were injected in the left retro-auricular region of the patients (Study Group). Three months after biopsies were harvested from this region, they were subsequently stained with Hematoxylin-Eosin and Picrosirius for comparative study between the two groups. Results: Statistical analysis of the number of collagen fibers in the three layers of the dermis - upper, middle and deep - comparing the study and control groups, showed that the mean and median observed after the injection of the cells were greater than those observed before the injection. Conclusion: The injection of fibroblasts results in an increase in the amount of collagen fibers in all regions of the dermis, with the increase being greater in the deeper regions.
Keywords: FIBROBLASTS; CELL-AND TISSUE-BASED THERAPY; COLLAGEN
The factors that trigger skin aging can be intrinsic (or chronological) or extrinsic. The first correspond to a natural process and are linked to genetic factors, a shortening of the telomeres, and the action of free radicals. 1 The second correspond to photoaging, which is the effect of solar radiation on intrinsic factors. 2 The main characteristics of the aging process of skin are: the thinning of the epidermis, the decrease in the number of dermal cells, the break up of collagen fibers, 3 the reduction of precursors of collagen types I and III, the reduction in the number of fibroblasts, and the hyperplasia of the elastic tissue. 4
The skin is the largest organ of the human body and, depending on the region, has variations in its thickness. 5 The dermis is mainly composed of fibroblasts - that produce collagen types I and III, and elastic fibers - and an extracellular matrix. This layer is responsible by the tonicity, elasticity and firmness of the skin. The dermis can be divided into superior, medium, and deep (or inferior) layers, with the highest concentration of fibroblasts and collagen fibers in the superior region. 6
In order to witness the explained concepts as regards the dermis, histological techniques of staining are used. More specifically, the hematoxylin-eosin technique (HE) is the most common and routine and allows the visualization of the collagen fibers in pink, while a picrosirius red is used for more specific analyses, staining the collagen in pink and red, making it very important for the analysis of results after specific treatments, as is the case of the objective of the present study. 7
The objective of the present prospective, comparative, controlled clinical study was to examine whether there is an increase in the production of collagen fibers in the human dermis after the injection of autologous fibroblasts in the skin of the retroauricular region.
The present study was approved by the Research Ethics Committee of the Universidade Santo Amaro (Unisa) under the protocol 030/2009.
Four Caucasian, non-smoking women, between the ages of25 and 60, originally from the Brazilian State of São Paulo, who wished to undergo aesthetic treatments on the face were selected. Local anesthesia was carried out with lidocaine without a vasoconstrictor, with the am of removing skin specimens from the right retroauricular region. Two skin biopsies were performed in each woman with 5 mm punctures. One of the fragments was taken to the cell culture laboratory and the other placed in a tube containing formalin and sent for histological analysis, and served as the control-group material. The specimens were stained with HE and picrosirius (F3BA sirius red staining in picric acid saturated solution, SPLABOR, SP, Brazil) for the evaluation of collagen fibers.
Fibroblasts extraction and cultivation process
The collected fragments were washed with 1% PBS (Phosphate Buffer Solution, LGC®, Cotia, SP, Brazil) and PS (penicillin streptomycin, LGC®, Cotia, SP, Brazil).
The fragments sent to the cell culture laboratory were transferred to the enzyme solution DPBS and EDTA (Hyqtase Hyclone®, Logan, Utah, USA), and remained in it for four hours. Subsequently, the dermis was mechanically separated from the epidermis and hair follicles. After the removal of the epidermis, the cellular explant of the dermis was carried out. For this purpose, the fragments were transferred to 25cm3 culture bottles and incubated for 30 minutes at 37ºC with 5% CO2. After this procedure, 5 ml of culture medium containing L-amino acids, Earle's salts and sodium bicarbonate (M199-LGC®, Cotia, SP, Brazil) were added and supplemented with 10% fetal bovine serum. The material obtained was sent for cultivation at a temperature of 37ºC, 5% CO2 and humidified air. 8
The cultured cells underwent the first changes of culture medium every two days up until reaching cell expansion. After this period, the culture medium was changed every four days. When 70% of primary confluence was achieved in the primary culture, the cells were treated with 0.25% trypsin enzyme (LGC®, Cotia, SP, Brazil), washed three times with PBS and centrifuged at 1,500 rpm for five minutes. The cell pellet was re-suspended with 1 ml of M199 and 20% of bovine fetal calf serum, and was then transferred to a 75cm3 bottle, with this procedure being considered the first doubling passage (1dp). The expansion of the fibroblasts was performed up until the third passage (3dp). The last change of medium in 3dp (already in 70% confluence of fibroblasts) was carried out with M199 supplemented with 20% of autologous serum.
After the trypsinization phase, the cell viability was carried out, with the cell pellet being subsequently re-suspended in 4 ml of PBS and divided into 10 syringes for injection (each containing fibroblast solution immersed in 0.4ml of PBS). That process had a total duration of eight weeks, after which the phase of injection of the solution in the patients' skin took place.
After the asepsis of the left retroauricular region and other areas, topic anesthetic cream with 4% lidocaine (Dermomax®, Lab Aché, SP, Brazil) was applied for 30 minutes, with the injection of fibroblasts (with 1ml syringes and 27G1/2 needles) being subsequently performed. One syringe was used for injection in the left retroauricular region (defined as the researched group's area), mainly in the medium and deep dermis. The remaining syringes were applied in the frontal and perioral rhytids, in the nasogenian folds, genian lips and periorbital skin, for the general treatment of the face.
Three months after the injection of fibroblasts, two fragments of the left retroauricular region (the study group area) were removed with punctures towards the tragus line, for comparison of the collagen fibers with those of the control group.
These fragments were also fixed in paraffin for the preparation of histological slides, having been stained with HE and picrosirius.
The slides prepared were used for quantifying and qualifying the collagen fibers, with the quantification performed using photographs taken with an Axion Vision 4, 2 REL camera (Carl Zeiss®) coupled to an Axiolab 2.0 microscope (Carl Zeiss®) and analyzed by the ImageLab 2000 software. Photographs were taken for analysis of the superior, medium, and inferior dermis of the control and research slides, in order to obtain the average percentage of collagen present in the tissue before and after the infusion of fibroblasts.
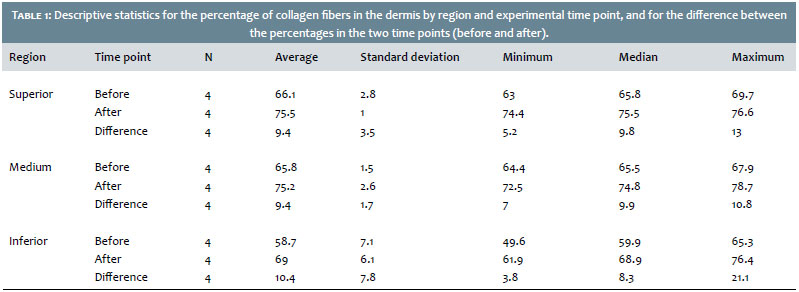
Descriptive statistics (mean, standard deviation, minimum, median and maximum values) were calculated from the percentage of collagen fiber in the periods before and after the application of the cells in the three regions of the dermis.
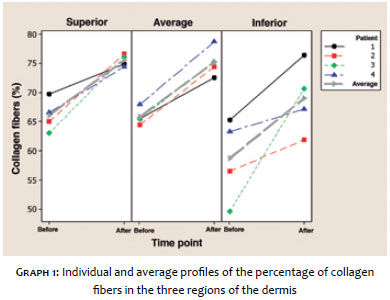
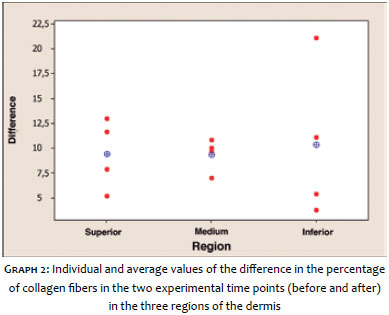
The individualized profiles of the percentage of fiber in the regions were represented graphically. A graph was prepared with the individualized values of the percentage differential between the experimental time points (before and after).
The paired t-test (Fisher and van Belle) was used to compare the mean values of the percentage of fibers in the two periods, for each region of the dermis. An alternative unilateral hypothesis was considered (higher average in the post experimental time point as compared to the pre experimental time point). The hypothesis test was performed with a significance level of 0.05.
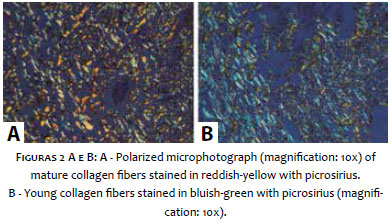
In the qualitative analysis, the different colors (in yellow and red for mature collagen fibers, and green for young collagen fibers) were compared between the control and research slides with photographs of these histological pieces having been obtained with the aid of an Axion Vision 4, 2 REL camera (Carl Zeiss®) coupled to a polarized microscope Axiolab 2.0 (Carl Zeiss®).
In the third passage (3dp) an average of 10 million cells was obtained, which were separated in ten syringes containing approximately 1 million cells each, with one of them being applied into the patients' left retro-auricular region.
Table 1 presents the observed values for the descriptive statistics of the percentage of collagen fibers by dermis region and experimental time point, and for the difference between the percentages in both periods (before and after). It is possible to notice that the mean and median observed after the application of the cells are higher than those observed before. The mean values and medians of the differences have the same magnitude in the three regions of the dermis. It is also possible to observe that the variability of the measurements (measured by the standard deviation) is greater in the inferior region.
The individual and average values of the percentages in the two experimental time points in the three regions of the dermis are represented in Graph 1. It is possible to observe that the values seen in the after experimental time point are greater than those in the before time point in all individuals, in the three regions. This result can also be seen in Graph 2, which includes representations of the individual and mean values of the percentage difference in collagen fibers in both periods (before and after).
The paired t test showed a significant difference between the average percentage of collagen fibers in the two periods, with the mean value in the after time point being greater than that of the before time point, in the superior (p = 0.006), medium (p = 0.001) and inferior (p = 0.039) regions.
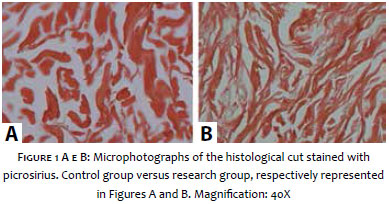
The birefringence qualitative assessment of the control and research group's dermis is presented in the form of microphotography. In the control group's images, it was possible to observe a large amount of mature collagen fibers stained in reddish yellow as compared to young fibers, which were stained in green, as shown in Figure 1.
In the research group it was possible to observe an increase in the amount of young collagen type III fibers stained green, as shown in Figure 2.
Skin thickness is mainly related to the layers of collagen and elastic fibers that constitute the dermis. 9
Cutaneous aging 10 causes a reduction of the skin's thickness and tone, contributing to the appearance of sagging, wrinkles, and frown lines, which are aggravated by external factors, such as solar radiation and smoking habits that accelerate the natural process of cutaneous aging. Among the many signs caused by this effect, are the reduction in the number in fibroblasts and the inhibition in the production and breakage of collagen fibers.
The superior region of the dermis has a greater amount of fibroblasts as compared to other regions and, consequently, a greater amount of collagen fibers11, a fact that was proved in the present study after the analysis of the control group's dermis samples.
The analysis of the three dermis layers of the control and research groups has shown that after applying fibroblasts there was an increase in the amount of collagen fibers in all regions, nevertheless the increase of these fibers in the inferior region was considerably large, promoting an amount of fibers proportional to that of the superior region.
This pattern of an increased number of collagen fibers was evidenced in all samples of the research group. According to the results of the birefringence analysis, the present study shows that the application of autologous fibroblasts promoted an increase in the amount of collagen fibers 12 in the patients' dermis, a fact that could be observed based on the increase in the number of young fibers, seen in the microphotographs of the polarized image.
The choice for the retroauricular region was due to the fact that it is less likely to be exposed to environmental effects 13 and not be aesthetically visible.
Recent studies with cultured fibroblasts can identify which substances are better at stimulating the activation genes to produce collagen. 14, 15 Fibroblasts in human skin in vivo are activated when they experience trauma of any kind, with the intention of repairing the damaged wall, as it occurs in chemical peelings, 16-18 lasers, 19, 20 microneedling with fractional radiofrequency, 21, 22 focused ultrasound, 23, 24 etc. Nonetheless, the authors did not find studies that showed, from a histological point of view, the dermis' region in the untouched skin after the application of human autologous fibroblasts. Despite the fact that several studies describe the action of cultured fibroblasts in the production of collagen fibers, there are no references to those injected into human skin.
In keeping with the birefringence results, the analysis of the three layers of the dermis of the research group showed an increased amount of collagen fibers in all layers after the application of fibroblasts.
1. Araujo TS, Souza SO. Protetores solares e os efeitos da radiação ultravioleta. Scientia Plena. 2008;4(11):1-7.
2. Moi, Regina C. Envelhecimento do sistema tegumentar: revisão sistemática da literatura. 2004. [Dissertação]. Universidade de São Paulo. Escola de Enfermagem de Ribeirão Preto. Ribeirão Preto; 2004. 111p.
3. Fisher GJ, Kang S, Varani J, Bata-Csorgo Z, Wan Y, DattaS, et al. Mechanism Photoaging and Chronological Skin Aging. Arch Dermatol. 2002;138(11):1462-70.
4. Skin rejuvenation with photodynamic therapy: collagen andelastic fiber analysis, and clinical improvement. SurgCosmetDermatol. 2010;2(2):87-92.
5. Rodrigues MM, Souza MS, Silva JL. Systematization of nursing care to prevent pressure-related tissue injury. CogitareEnferm. 2008;13(4):566-75.
6. Scheuplein RJ. Permeability Of The Skin. ComprehensivePhysiology. 2011;2:456-71.
7. Manela-Azulay M, Cuzzi T, Pinheiro JCA, Azulay DR, Rangel GB. Métodos objetivos para análise de estudos em dermatologia cosmética. Na Bras Dermatol. 2010;85(1):65-71.
8. Eça LPM, Pinto DG, Murari ASP, Mazzetti MPV, Odo M. Autologous Fibroblast Culture in the Repair of Aging Skin. Dermatol Surg. 2012;38(2):180-4.
9. Fathi-Azarbayjani A, Tan PL, Chan YY, Chan SY. Ascorbic Acid for the Safe Use of a Sunscreen Agent: Accumulation of Nano Zinc Oxide and Titanium Dioxide on the Skin. Sci Pharm. 2013;81(4):1141-50.
10. Oriá RB, Santana EN, Fernandes MR, Ferreira FVA, Brito GAC. Study of age-related changes in human skin using histomorphometric and autofluorescence approaches. An Bras Dermatol. 2003;78(4):425-34.
11. Osman SO, Selway JL, Harikumar PE, Stocker CJ, Wargent ET, Cawthorne MA, et al. A novel method to assess collagen architecture in skin. BMC Bioinformatics. 2013;14:2-10.
12. Boss WK, Usal H, Fodor PB, Chernoff G. Autologous cultured fibroblast: protein repair system. Annals of Plastic Surgery. 2000;44(5): 536-42.
13. Jolivot R, Benezeth Y, Marzani F. Skin Parameter Map Retrieval from a Dedicated Multispectral Imaging System Applied to Dermatology/ Cosmetology. Inter J Biomed Imag. 2013;2013:978289.
14. Avantaqqiato A, Girardi A, Palmieri A, Pscali M, Carinci F. Comparison of Bio-Revitalizing Injective Products: A Study on Skin Fibroblast Cultures. Rejuvenation Res. 2015;18(3):270-6
15. Bygd HC, Akilbekova D, Muñoz A, Forsmark KD, Bratlie KM. Poly-L-arginine based materials as instructive substrates for fibroblast synthesis of collagen. Biomaterials. 2015;63:47-57.
16. Omi T, Sato S, Numano K, Kawana S. Ultrastructural changes of the skin due to chemical peeling. J Cosmet Laser Ther. 2010;12(1):21-4.
17. Hexsel D,Mazzuco R, Dal'Forno T, Zechmeister D. Microdermabrasion followed by a 5% retinoic acid chemical peel vs. A 5% retinoid acid chemical peel for the treatment of photoaging- a pilot study. J Cosmet Dermatol. 2005;4(2):111-6.
18. Monheit GD. Medium-depth chemical peels. Dermatol Clin. 2001;19(4):413-25.
19. Brauer JA, Kazlouskaya V, Alabdulrazzaq H, Bae YS, Bernstein LJ, Anolik R, et al. Use of a picosecond pulse duration laser with specialized optic for treatment of facial acne scarring. JAMA Dermatol. 2015;151(3):278-84.
20. Stuzin JM, Baker TJ, Baker TM, Kligman AM. Histologic effects of the high- energy pulsed CO2 laser on photoaged facial skin. Plast Reconstr Surg. 1997;99(7):2036-50.
21. Lee HJ, Seo SR, Yoon MS, Song JY, Lee EY, Lee SE. Microneedle fractional radiofrequency increases epidermal hyaluronan and reverses age-related epidermal dysfunction. Lasers Surg Med. 2015 sep 28. doi: 10.1002/lsm.22420. [Epub ahead of print]
22. Hantash BM, Ubeid AA, Chang H, Kafi R, Renton B. Bipolar fractional radiofrequency tratment induces neoelastogenesis and neocollagenesis. Lasers Surg Med. 2009;41(1):1-9.
23. Suh DH, Choi JH, Lee SJ, Jeong KH, Song KY, Shin MK. Comparative histometric analysis of the effects of high-intensity focused ultrasound and radiofrequency on skin. J Cosmet Laser Ther. 2015;17(5):230-6.
24. MacGregor JL, Tanzi EL. Microfocused ultrasound for skin tightening. Semin Cutan Med Surg. 2013;32(1):18-25.
The present study was conducted at the Instituto de Pesquisa de Células Tronco (IPCTRON) and at the Laboratório de Histologia da Universidade Federal de São Paulo - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}