


Fernanda Freitas de Brito1; Tatiana Cristina Pedro Cordeiro de Andrade2; Ana Paula Cota Pinto Coelho3; Ana Cecília Versiani Duarte Pinto1; Adauto José Ferreira Nunes4; Claudio Sampieri Tonello4
Lichen sclerosus is an uncommon condition affecting both the genital and extragenital region, the latter constituting an atypical occurrence of the disorder. The use of topical corticosteroids is considered the first-line treatment of this genital disease. Extragenital lesions are less sensitive to this therapy. The present study describes a case of lichen sclerosus in an 82-year-old female patient, with widespread extragenital involvement and successful treatment with narrow band UVB phototherapy. Lichen sclerosus is a chronic inflammatory dermatosis and disseminated forms of the condition are rare, with an absence of consensus on the treatment of the extragenital form. The choice for narrow band UVB therapy was based on the literature.
Keywords: LICHEN SCLEROSUS ET ATROPHICUS; ATROPHY; PHOTOTHERAPY
Lichen sclerosus (LS) is an uncommon condition with a 0.1-0.3% prevalence, mainly affecting prepubescent and post-menopausal women.1-3 It affects both the genital and extragenital region, the latter being an atypical presentation of the disorder.3-6 In men, it primarily affects the glans and can be the cause of phimosis.1, 3 The etiology is unknown, though evidence suggests that immunological mechanisms are involved in its pathogenesis due to association with other autoimmune diseases such as pernicious anemia, vitiligo, morphea, and autoimmune thyroiditis. Genetic factors and alterations in the androgens metabolism were also associated with this pathology.1, 2, 5, 6 It clinically manifests as hypochromic, atrophic, and bright plaques, asymptomatic or pruritic.1 The extragenital form of LS occurs in 15-20% of cases when associated with the genital form,1, 5, 6 while the isolated extragenital form is very rare, appearing in only 2.5% of all cases.1 It generally occurs in the upper area of the trunk, armpits, buttocks, and thighs 1-3, 5. The diagnosis is clinical and is confirmed by specific histological pattern.2,3
For the treatment of LS, the use of potent topical corticosteroids is considered a first line therapy in the genital lesions.1-3, 5 Extragenital lesions are less sensitive to conventional therapy.1, 3 There are, however, reports on the use of tacrolimus,2, 3, 5 colchicine,2, 3 cyclosporine,3 methotrexate, mycophenolate mofetil and a number of phototherapy modalities (narrow band UVB, UVA-psoralen, UVA-1).4, 5 The present case report aims at presenting a rare form of LS, with widespread extragenital involvement and successful treatment with narrow band UVB phototherapy.
Case report
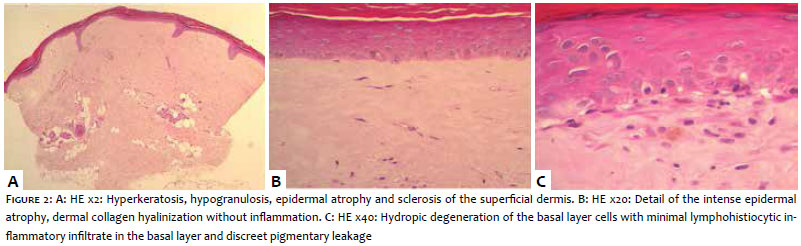
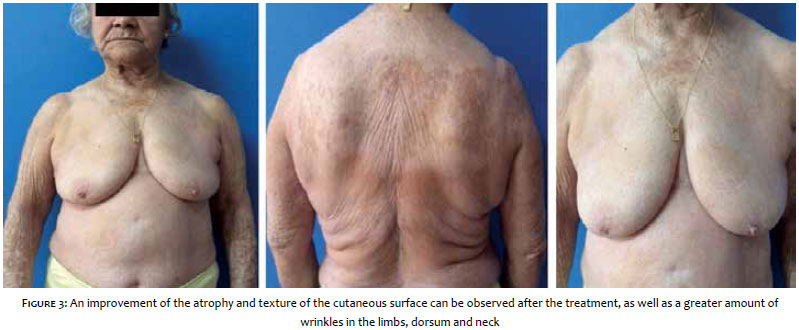
An 82-year-old female patient, with an eight-month history of the appearance of hypochromic and atrophic plaques spread widely over the body. She denied any systemic symptoms or weight loss. Dermatological examination showed extensive hypochromic plaques with bright and atrophic surfaces, affecting the cervical, upper trunk, abdomen, and dorsum regions, arms and legs. There was an absence of genital involvement (Figure 1). Two biopsies of the lesions located in the dorsum showed hyperkeratosis, hypogranulosis, marked atrophy of the epidermis, hyalinization of the dermis' collagen with discreet lymphohistiocytic infiltrate, all compatible with LS (Figure 2). Symptomatic treatment was started with antihistamines. Due to the extent of the lesions, topical corticosteroids were not prescribed. A decision was then made for narrow band UVB phototherapy. The patient underwent 16 sessions, with an irradiation dose that ranged from 580 to 1,840mJ/cm2 per session, with a total dose of 24,540mJ/cm2 and an exposure time of 3 to 10 minutes per session. A significant improvement in the pruritus and the clinical picture was observed after five months of treatment, with improved atrophy and cutaneous surface texture (Figure 3). The phototherapy was suspended, and the patient receives regular follow up by the service.
LS is a chronic inflammatory, uncommon dermatosis,1 first described in 1887 by Hallopeau.1 It is characterized by pearly-white plaques, which can be arranged in groups and progressively assume the aspect of parchment skin. Disseminated forms of the disorder are extremely rare.5 In the present case report, the patient has an unusual form of LS, with the presence of generalized hypochromic and atrophic plaques affecting most of the tegument, except for the face, palmoplantar regions, scalp, oral, and genital mucosa. When there is genital involvement, the first line of treatment is with topical corticosteroids.3, 5 Nevertheless, regarding the treatment of the extragenital form, there is no consensus in the literature,3 which in general is composed of individual cases and small case series. The guidelines of the British Association of Dermatology make reference to various treatments, all with a low level of scientific evidence.3 Topical treatments with high potency corticosteroids were not considered in the present case due to the extent of the affected area. Various forms of phototherapy have been used successfully. The choice for narrow band UVB therapy was based on published reports,4, 5 as well as on the availability of equipment in the authors' institution. Five months after completing treatment with 16 sessions, the patient showed significant improvement of the pruritus - the main complaint - and also in the clinical appearance of the lesions. A case report published in 2007 by Colbert et al.5 showed a similar result. Phototherapy promotes the release of cytokines that induce formation of collagenase and inhibit the synthesis of collagen, in addition to its immunosuppressive effect.4, 5, 7 According to the literature, other therapies that must be considered in extensive lesions include methotrexate, hydroxychloroquine, cyclosporine, and mycophenolate mofetil.3 Due to the limited availability of randomized trials and large cohort studies, it is difficult to draw definitive conclusions about the effectiveness in the long run of narrow band UVB phototherapy,5, 7 the optimum dose, and better treatment schemes. However, evidence based on case reports has shown good results, and this treatment looks promising in the management of extragenital LS.1
1. Trinh TVT, Parr K, DF. Disseminated extragenital bullous lichen sclerosus. Indian Dermatol Online J. 2014;5(1):66-68.
2. Fonseca JSBM, Silva AGF, Guimarães MG, Faria PA, Filho FB. Líquen escleroso extragenital com resposta à colchicina. Revista SPDV. 2013;71(2):273-6.
3. Neill SM, Lewis FM, Tatnall FM, Cox NH, Dermatologists BAo. British Association of Dermatologists' guidelines for the management of lichen sclerosus. Br J Dermatol. 2010;163(4):672-82
4. Kreuter A, Gambichler T. Narrowband UV-B phototherapy for extragenital lichen sclerosus. Arch Dermatol. 2007;143(9):1213.
5. Colbert RL, Chiang MP, Carlin CS, Fleming M. Progressive extragenital lichen sclerosus successfully treated with narrowband UV-B phototherapy. Arch Dermatol. 2007;143(1):19-20.
6. Coelho WS, Diniz LM, Souza Filho JB. Líquen escleroso e atrófico - relato de dois casos de apresentação atípica. An Bras Dermatol. 2006;81(5):297-300.
7. Duarte I; Buense R; Kobata C. Fototerapia. An Bras Dermatol. 2006;81(1):74-82.
This study was carried out at Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}