


André Cesar Antiori Freire Pessanha1; Luiz Roberto Terzian2; Fernanda de Sousa Ferrara3
Lip cancer corresponds to 25-35% of all oral cancers. Squamous cell carcinoma is the most common histological type in this location (95%). Various wound reconstruction options are described for the exeresis of this type of tumor in the lower lip - the choice depending on the surgeon's experience and the proportion of the final defect regarding the dimensions of the lip. The present article describes the case of a male patient with a wound in the lower lip that was histologically diagnosed as an invasive squamous cell carcinoma. Mohs surgery was implemented and a transposition flap (Abbé flap) was used in the reconstruction of the upper lip. The complete opening of the mouth, without functional impairment of the speech or chewing function, and a favorable aesthetic result, were observed in the follow-up, thus demonstrating the usefulness of this type of reconstruction.
Keywords: MOHS SURGERY; CARCINOMA, SQUAMOUS CELL; RECONSTRUCTION
Lip cancer corresponds to 25-35% of all oral cancers. Squamous cell carcinoma (SCC) is the most common histological type in this location (95%), and is 20 times more prevalent in the lower lip than in the upper lip, affecting more men than women (6:1) and more often those over 50 years, with fair-skin, and those engaged in professions that require chronic exposure to ultraviolet radiation. It is uncommon in younger people, however the chances increase if they are HIV-infected or have undergone a kidney transplant. When diagnosed at an early stage, the cure rate is 80-90%, with a mortality rate ranging from 10-15%. Metastases vary from 11-18%, and in such cases the five-year average survival rate falls to 25%.1
There are several options for wound reconstruction after SCC resection in the lower lip, depending on the surgeon's level of experience and the proportion and dimensions of the of final defect in relation to the size of the lip. Defects that take up half of the lip can be rebuilt using the W-plasty or a rectangular flap. Defects taking up 1/2 to 2/3 of the lip depend on the involvement or not of the labial commissure. If the commissure is affected, the Estlander flap is indicated, if not, the Abbé flap should be used. Wounds involving 2/3 of the lip or greater will be rebuilt according to the location of the defect. If it is centrally located, the Bernard-Burrow-Webster flap is indicated; if it is laterally located, the Gate or Karapandzic flaps are better options.2
Case report
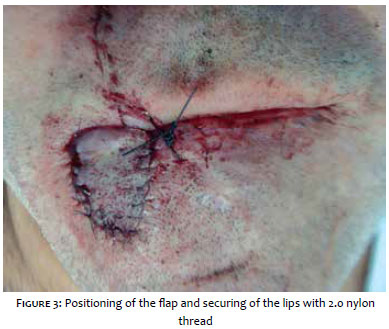
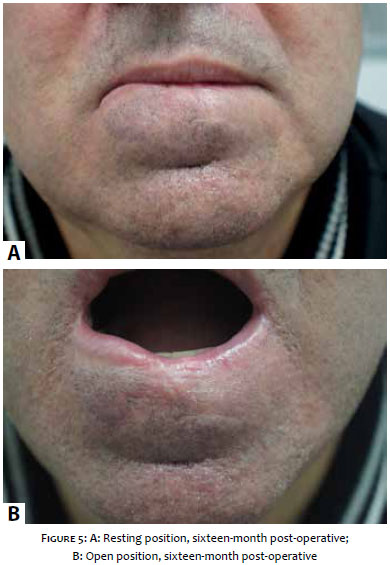
A 56-year-old male patient, born in the city of Santo André (SP, Brazil) had a wound on the lip for six months, with progressive development. He had already undergone a tumor operation in the same location in 2010. The dermatological exam showed ulcerovegetative tumoration with a bleeding surface and meliceric crusts, accompanied by a foul odor (Figure 1). The cervical lymph nodes were not palpable. The pathological examination evidenced invasive SCC, with a moderate degree of differentiation (Broders II). The patient underwent Mohs micrographic surgery according to the following criteria: SCC, large dimensions and involvement of the free edges, in addition to possible recurrence. Number of steps: 1. Number of fragments: 4. Reconstruction technique: transposition flap of the upper lip - Abbé flap (Figures 2 and 3). The nutrition pedicle was kept for three weeks, during which a liquid and soft diet was administered, with the pedicle having been sectioned at the end of that period (Figure 4). The complete opening of the mouth was eventually possible, without functional impairment of speech or mastication, and with a favorable aesthetic result. (Figure 5)
In 1898, Abbé described a flap involving the transfer of a total thickness triangular segment of the tissue of the lower lip to a full-thickness defect in the upper lip. This type of reconstruction is ideal for defects covering from 2/3 to 100% of the lip.3-5 It is the ideal choice for lateral defects the in lower lip that cannot be closed with advancement and rotation flaps.6 The flap is drawn with a size corresponding to half of the size of the defect and is rotated on an axis almost 180º over the pedicle as it is inserted into the defect on the opposite side. The pivotal point is fixed near the commissure in order to keep a more proximal irrigation.4 This insertion is enhanced by an anchoring stitch with 2.0 nylon thread so that nutrition is not compromised by the movements of the lip and in order to avoid a possible rupture of the pedicle. While the flap is in this position, patients can have a limited oral diet with liquids and soft foods that do not require biting or chewing. After three weeks the pedicle, as well as the 2.0 nylon stitch, is ruptured.3
In most cases, the height of the opposite side flap is designed to match that of the receiving location, with a width corresponding to half of the defect's width.3
The main source of nutrition for the Abbé flap is the labial artery, 3 which is a branch of the facial artery. It originates in the deep layers of the orbicularis oris and depressor of the mouth's angle muscles. Its path goes between the labial mucosa and the orbicularis muscle, topographically corresponding to the posterior line of the vermilion.5 It tends to become slightly more cephalic in the central region of the upper lip. Therefore, it is safer to use a lateral pedicle when the flap is extracted from the upper lip. The skin incision that creates the flap can extend up until the distance limited by the anterior portion of the vermilion.3 It is important to rigorously approximate all layers of the lip with sutures - especially the muscle - in order to avoid the formation of a depressed and uneven scar around the flap's border.3
1. Vieira RAMAR, Marques MEA, Minicucci EM, Marques SA; Actinic cheilitis and squamous cell carcinoma of the lip: clinical, histopathological and immunogenetic aspects; An Bras Dermatol. 2012;87(1):105-14.
2. Craigg L. ; Operative techniques in otolaryngology- Head Neck Surg. 1993;4(1):46-53.,
3. Baker SR. Retalhos locais em reconstrução facial. 2ª ed. Rio de Janeiro: DiLivros; 2009
4. Baumann D, Robb G. Lip reconstruction. Semin Plast Surg. 2008;22(4):269-80.
5. Sajjadian A, Narayan D. Lip reconstruction procedures. Acessado em : 30/03/2014. Disponível em: http://emedicine.medscape.com/article/1288447-overview#a04
6. Boutros S, Reconstruction of the lips, Grabb and Smith's Plastic Surgery, Sixth Edition, Copyright©; 2007.
This study was carried out at the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}