


Sandra Lopes Mattos e Dinato1; Glaucia Pereira Christo Antonioli2; José Roberto Paes de Almeida3; Ney Romiti (In memorian)4; Nelson Mattos Tavares5
Endometriosis is a common dermatosis that most typically affects the pelvic organs. Extra-pelvic occurrences are reported in the literature. Umbilical endometriosis is rare and can be primary (spontaneous) or secondary (after surgery). The present study describes the case of a female patient with endometriosis lesions in the umbilical region, confirmed by histology. Treatment was carried out with wide surgical excision. It is important to note that differential diagnosis should be considered in the presence of umbilical tumors in women of reproductive age.
Keywords: ENDOMETRIOSIS; SISTER MARY JOSEPH'S NODULE; ABDOMINAL NEOPLASMS; ABDOMINAL WALL; ADENOMYOSIS
Endometriosis is characterized by the presence of ectopic implantation of endometrial glands and stroma, typically functional and sensitive to hormones.1-5 It is a common disorder, usually chronic and benign, that affects the pelvic organs.1-4 The most frequent focus is the ovary.4, 5 It affects around 5-10% of women of reproductive age,1, 3 however it can also occur in women at menarche and menopause.1, 2 It is an exception in men, occurring after long-term hormone therapy for prostatic tumors.1 Extrapelvic onset of endometriosis can occur in about 12% of women with the disorder.2, 6
The incidence of umbilical endometriosis is infrequent - about 0.5-1.0% of the total cases.5-8 Studying 4,376 cases of endometriosis, Fernandez-Aceñero and Córdoba found only two with an umbilical location (0.53%). It can be classified into primary (spontaneous)2-4 or secondary (after surgery). The primary form is even less common.2 The rarity of this cutaneous presentation was the reason for the present paper.
A 24-year-old mullato female patient, married, housewife, originally from the city of Sorocaba (Brazilian State of São Paulo State), living in the city of São Vicente (Brazilian State of São Paulo State). She describes the appearance of a lesion in the umbilicus three years before, with a slow and progressive growth, and increased sensitivity during the onset of menstrual periods. The patient denies bleeding and having undergone previous abdominal surgeries.
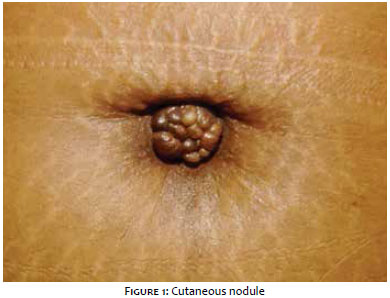
Dermatological examination revealed a nodular lesion with vegetating aspect and convoluted surface, circular in shape, 1.5 cm in diameter and reddish-violet in color, with a firm consistency (Figure 1).
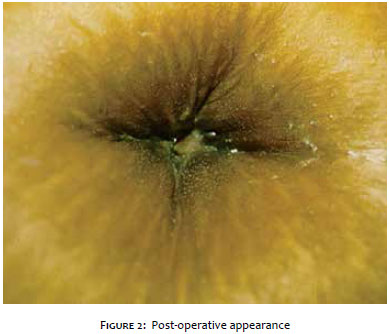
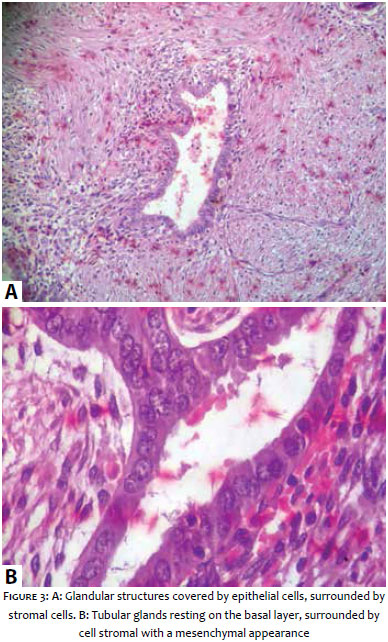
Surgical exeresis of the entire lesion was performed (Figure 2) and the histological examination (Figure 3A and 3B) showed simple tubular glandular structures, covered with a single or double layer of uniform epithelial cells, resting on a basal layer surrounded by cell stroma, with mesenchymal aspect, and a presence of intercellular ground substance. These findings are compatible with glands and endometrial stroma, confirming the diagnosis of cutaneous endometriosis. It is worth noting that the complete removal of the nodule showed satisfactory cosmetic results, without the need for reconstructive surgery of the navel. It is also important to note that no other previous tests, such as a biopsy, ultrasound, or magnetic resonance, were carried out because a choice was made for the immediate complete surgical resection, given that the dimensions of the lesion allowed for the procedure to be performed.
Due to the fact that it is a systemic disorder, the patient was referred for follow up with the gynecology sector, and warned about the possibility of recurrence. The development was asymptomatic. There was an absence of alterations of the clinical picture during a 2-year ambulatorial guidance and follow up. After that period, the patient did not return to the hospital.
Extrapelvic endometriosis may compromise diverse organs of the human body. The most common locations, in descending order, are the intestines, skin (including the navel and abdominal scars), inguinal and thigh regions, lungs and pleura, pancreas, meninges, and vertebrae.7
Umbilical endometriosis
In general, cutaneous and subcutaneous involvement is secondary to healing processes after abdominal and/or pelvic surgeries, such as laparoscopy/laparotomy, cesarean section, hysterectomy, metroplasty, myomectomy, episiotomy, appendectomy, cyst removal from the Bartholin gland, amniocentesis, and intrauterine injections for abortion.1-3, 6, 7, 9
Fewer than 30% of endometriosis cases emerge in the absence of surgery and are referred to as primary or spontaneous cutaneous endometriosis,3, 4 as occurred with the studied patient, who has never undergone abdominal surgery.
Despite its low incidence rate, the umbilicus is the most common primary site, as reported in the present case.3, 7, 9 Other primary cutaneous sites include the vulva, perineum, groin, and extremities.7 It can also develop during pregnancy, most often in the umbilical region, and can have spontaneous regression after delivery.5
Several theories attempt to explain the development of endometriosis, however the pathogenesis remains unclear. In transtube regurgitation theory, the ectopic endometrial tissue is conveyed by retrograde menstruation to the site where the endometriosis is installed. In the mechanical transplantation theory, the intra-abdominal implant of endometrial cells occurs via lymphatic vessels, vascular propagation or by displacement of endometrial tissue during surgery (such as laparoscopic procedures), the main hypothesis for cutaneous endometriosis. In the coelomic metaplasia theory, the ectopic endometrium develops from a hormonal estrogenic stimulus in cells of the same embryonic origin. And lastly, in the decreased immune response theory, in which the reduction of the natural immune system attack activity causes decreased depuration of endometrial cells in the peritoneal cavity.1, 3, 8 The cutaneous endometriosis of the navel/umbilical scar manifests as a nodule with firm consistency, measuring 2.0-2.5 cm and variable color (from bluish-black to brown or deep red, depending on the amount of bleeding and depth of penetration of the ectopic endometrial tissue). Occasionally, the nodule is skin color.1, 8, 9 They are typically single in number and often multi-lobulated, although multiple discrete nodules may be present.7 Clinical symptoms include pain, hyperesthesia, bleeding, edema, and growth correlated with the menstrual cycle.1,7 However, all symptoms are rarely present at the same time, and it may even be asymptomatic, as in the present case.8, 9 Hemorrhage related to menstrual bleeding is absent in most cases.4
Gynecological symptoms, such as dysmenorrhea, dyspareunia, infertility, and menstrual irregularities are generally present in the pelvic endometriosis and absent in the skin endometriosis.1, 7 The most common differential diagnoses include pyogenic granuloma, hernia, and vegetating pemphigus. Due to the variable macroscopic appearance, these lesions may also be initially mistaken with malignant tumors, such as melanoma.1, 3-5, 8 Recent reports have shown that magnetic resonance3 and dermoscopy can be helpful in differentiating umbilical endometriosis and other pigmented skin lesions.3, 6, 8 Correlated dermoscopy and histopathology can be complementary and efficient for diagnostic clarification,6 nevertheless there are not enough studies supporting its superiority as compared to histopathology.
In this way, the gold standard diagnosis is confirmed by histological examination.1, 4, 5, 7, 8 In the cutaneous lesions, irregular circular, angular, or elongated irregular glandular spaces can be observed in the reticular dermis or hypodermis, surrounded by highly vascular and cellular stroma, similar to that of the functioning endometrium.8, 10 The histological appearance corresponds to the uterine endometrium in the proliferative and secretory phases.10 Infrequently used in practice, the ultrasonography only indicates a hypoechogenic area with various sizes and irregular margins, which does not increase the precision of the information.6
Regarding the treatment, simple surgical excision is the first choice, and should be large enough to ensure the complete resolution of the condition.3-5, 7, 9 Prior hormonal treatment can be an option for larger tumors and can promote the reduction of their size before the surgery.10
The prognosis of cutaneous endometriosis is good and recurrences are uncommon. Nonetheless, malignant transformation has been reported as a percentage ranging from 0.3-1.0% of cases of endometriosis scars and should be suspected in recurring lesions or in the presence of rapid growth. The possibility of coexistence of genital with abdominal endometriosis, which worsens the prognosis, as well as modifies the treatment, should always be investigated. In this case, hormone therapy must be associated.7, 10 The studied patient did not have any recurrence or any complication after the surgery and during the two-year follow-up.
Umbilical endometriosis is therefore a rare disorder, however it should be considered in the differential diagnosis in cases of women of childbearing age who have lesions in the umbilical scar, even if asymptomatic. Definitive diagnosis is histologic, and surgical excision is the preferred therapy.
1. Kyamidis K, Lora V, Kanitakis J. Spontaneous cutaneous umbilical endometriosis: report of a new case with imunohistochemical study and literature reviw. Dermatol Online J. 2011;(15 Supll 7):5.
2. Choi SW, Lee HN, Kang SJ, Kim HO. A case of cutaneous endometriosis in postmenopausal woman receiving hormonal replacement. J Am Acad Dermatol. 1999;41(32):327-9.
3. Agarwal A, Fong YF. Cutaneous endometriosis. Singapore Med J. 2008;49(9):704-9.
4. 4 Fernández-Aceñero MJ, Córdova S. Cutaneous endometriosis: review of 15 cases diagnosed at a single institution. Arch Gynecol Obstet. 2011;283(5):1041-4.
5. Razzi S, Rubegni P, Sartini A, De Simone S, Fava A, Cobellis L, et al. Umbilical endometriosis in pregnancy:a case report. Gynecol Endocrinol. 2004;18(2):114-6.
6. De Giorgi V, Massi D, Mannone F, Stante M, Carli P. Cutaneous endometriosis: non-invasive analysis by epiluminescence microscopy. Clin Exp Dermatol. 2003;28(3):315-7.
7. Castro MCR, Costa APF, Salles R, Maya TC, Silva MR.Endometriose Umbilical. An bras Dermatol.1997;72(3):255-8.
8. Chatzikokkinou P, Thorfinn J, Angelidis IK, Papa G, Trevisan G. Spontaneous endometriosis in an umbilical skin lesion. Acta Dermatovenerol Alp Pannonica Adriat. 2009;18(3):126-30.
9. Fedele L, Frontino G, Bianchi S, Borruto F, Ciappina N. Umbilical endometriosis: a radical excision with laparoscopic assistance. Int J Surg. 2010;8(2):109-11.
10. Tidman MJ, MacDonald DM. Cutaneous endometriosis: a histopathologic study. J Am Acad Dermatol. 1988;18(2):373-7.
Trabalho realizado no Centro Universitário Lusíada (Unilus) - Santos (SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}