


Ana Cecília Versiani Duarte Pinto1; Maria Lopes Lamenha Lins Cavalcante1; Gardênia Viana da Silva2; Fernanda Freitas de Brito1; Agnes Mayumi Nakano Oliveira2; Norma Gondim Cleto3
Keywords: EPIDEMIOLOGY; MELANOMA; HISTOLOGY; PATHOLOGY, SURGICAL; SKIN NEOPLASMS
Melanoma is a malignant neoplasm arising from melanocytes that predominantly occurs in the skin (in over 90% of cases). However, it can also be observed in mucous membranes, on the eyeballs, or the leptomeninges. 1 In Brazil, cutaneous malignant melanoma (CMM) is aligned with the worldwide trend of an increasing incidence yet reduced degree of severity in diagnosed cases. 1-4 Despite being the most lethal skin cancer, 2, 5 the population from which epidemiological data from CMM cases can be collected in Brazil is limited, mainly due to the absence of mandatory reporting, the lack of central registration of cases, and little attention from public health managers. 6 In the present study, the authors used the prognostic criteria of the Brazilian Multicenter and Multidisciplinary Melanoma Study Group (Grupo Multicêntrico e Multidisciplinar Brasileiro para Estudo do Melanoma - GBM), 7, 8 for the preparation of clinical and histological profiles of CMM cases seen in the last seven years in dermatologic referral centers in the Southeast city of Bauru (SP). Thus, the objective of the study is to develop a profile corresponding to a risk group, encourage early diagnosis, and contribute to the targeting of prevention campaigns.
A cross-sectional descriptive study with retrospective analysis carried out using the medical records of all patients who had a histological diagnosis of primary CMM by excisional biopsy in a tertiary unit of the dermatology referral in the city of Bauru (SP), between January 2007 and July 2014.
The sampling was non-probabilistic for convenience, including all patients with histological diagnosis of primary cutaneous melanoma by excisional biopsy during the study period. Melanomas of mucous membranes and eyes, metastatic melanomas, residual melanomas, recurrent melanomas, melanomas observed in slides review or in incisional biopsies were excluded. In all, 64 cases of primary cutaneous melanoma were assessed.
For each case, the epidemiological and clinical characteristics were identified: age, gender, time elapsed between the lesion onset and diagnosis, and tumor location. The histological characteristics, such as melanoma subtype classification and GMB's prognostic criteria 7, 8 were also identified: Clark index, Breslow thickness, mitotic index, presence of lymphocytic infiltrate, presence of angiolymphatic and perineural invasion, presence of ulceration and regression, microscopic satellitosis and compromise of surgical margins.
Because the study was based on data collection from medical records and histological examinations, possible measurement and information bias should be considered.
The data were processed using Microsoft® Excel with frequency and percentage analysis, and preparation of graphs. The principles of the Declaration of Helsinki were observed during the study.
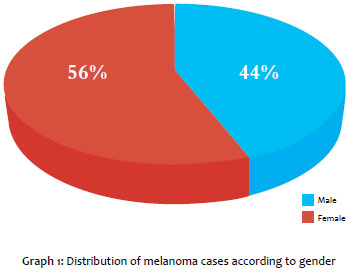
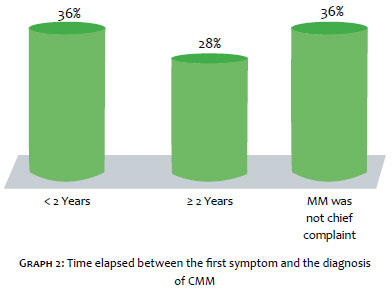
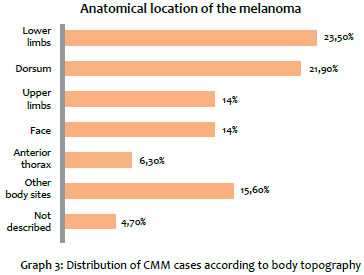
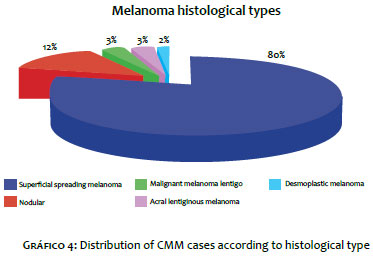
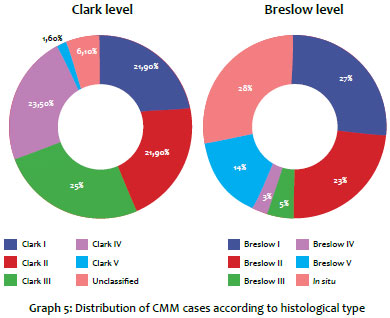
In the present study, 43.8% of patients were male, and 56.2% were female (Graph 1). The age of the sample ranged from 27 to 95 years (mean age = 61.4 years). The time elapsed between the lesion onset and diagnosis was fewer than 2 years in 36% of patients, longer than 2 years in 28% of patients, and for 36% of the patients the lesion was not the main complaint and was detected on physical examination (Graph 2). Regarding the lesions' topography, the most affected body sites were the lower limbs (23.5%), followed by the dorsum (21.9%), upper limbs and face (each with 14%), anterior chest (6.3%) and other sites (15.6%). In 4.7% of cases this datum was not included in the record (Graph 3). The superficial spreading type corresponded to 79.6%, the nodular type to 12.6%, the lentigo maligna melanoma and the acral lentiginous melanoma each corresponded to 3.1%, and the desmoplastic melanoma to 6.1% (Graph 4). Regarding the GMB's severity criteria, the Breslow thickness ranged from 0.12 mm to 37.0 mm (mean = 2.9 mm). In 28.1% of cases the lesion was in situ. The percentages of each thickness, Breslow (I to V) and Clark levels (I to V) are highlighted in Graph 5. The ulceration was present in 14.2%, regression areas in 26.6%, and mitotic index higher than zero in 34.4%. Only one case (1.6%) had angiolymphatic invasion, and 42.2% of biopsies showed lymphocytic infiltrate. Satellitosis and neural invasion were not detected. Regarding the compromise of surgical margins, the biopsies were free of neoplastic involvement in 81.3% of cases, while there was a presence of compromise in 15.6% of cases. This datum was not recorded in 3.1% of cases. Research in search of other skin cancers was positive in 43.8% of patients.
CMMs were more common in women (56.2%), consistent with studies conducted in the Brazilian states of São Paulo (Southeast Region) and Santa Catarina (South Region). 2, 3, 9-11 This association relates to women's greater adherence to prevention campaigns and more frequent use of healthcare services. The average age at diagnosis of 61.4 years is similar to that observed in a Portuguese study (61 years)1 and other Brazilian studies, such as those conducted in the city of Curitiba (South Region), with an average age of 58 years12 and in the city of Brasilia (Mid-West Region), with more cases affecting the age group of 61-80-year-olds. 13 Prevalence in the elderly is a result of increased life expectancy coupled with a greater difficulty in this age group for early detection of neoplastic lesions. In line with other studies, 6,14 the association of CMM with other skin cancers was verified at 43.2%, pointing towards a subgroup of individuals with intense exposure to the sun. In 36% of patients, although CMM was not the complaint leading to the consultation, this condition was detected during an examination. In this context, it is important to recognize the importance of a complete dermatological examination, which includes performing a dermoscopy. This is a non-invasive, ancillary diagnostic tool of high sensitivity (98.8%) and specificity (91.2%) for CMM detection, making it very important in the differentiation of melanocytic and non-melanocytic lesions. 14-16 The most affected topographies were the lower limbs (23.5%) and the dorsum (21.9%), consistent with the literature data. 1, 3, 4, 17, 18 Hospital-based publications of the 1990s and first decade of the century XXI 13, 19, 20 show a higher incidence of the nodular subtype with a lower proportion of non-invasive diagnosis of CMM. The present study confirms the emergence of a new profile for CMM in Brazilian tertiary units, with the superficial spreading type as the most frequent (79.6%) and 28.1% of lesions diagnosed in situ. Regarding GBM's severity criteria, most patients in the present study offered evidence of a good prognosis, with Breslow levels I and II in half of the cases, Clark levels I, II, and III in 68.8%, and a mitotic index greater than zero in only 34.4%. Moreover, other severity criteria such as regression, ulceration, and angiolymphatic invasion showed low positivity. Still, regarding the degree of severity there was no satellitosis and neural invasion. Most reports (81.3%) described free surgical margins, revealing technical diligence in excisional biopsies. Historically, severe cases of CMM prevailed in tertiary hospitals. 13, 19, 21 The present study shows that this scenario is changing, with a greater tendency toward early diagnosis. This early diagnosis profile combined with better prognosis was observed in other Brazilian studies conducted in the South and Southeast regions, 2, 3, 8, 22 However, this profile was not found in similar studies conducted in the North and Northeast regions, 6, 17 a fact that reveals important regional differences that must be considered when planning prevention campaigns for the population.
In this study, the following CMM profile was observed: female, average age = 61 years, with lesions not always observed before the consultation, located in lower limbs or trunk, with superficial spreading subtype and with good prognostic signs according to the GBM's criteria. Studies such as the present paper, which strives for the identification of risk groups, prognostic factors, and the understanding of CMM histological behavior, are important for providing subsidies for the design of strategies for approaching populations.
Acknowledgements:
The authors would like to thank the doctors and staff of the pathology laboratory of the Instituto Lauro de Souza Lima, in Bauru (SP), Brazil.
1. Moreira J, Moreira E, Azevedo F, Mota A. Melanoma maligno cutâneo: estudo retrospectivo. Acta Med Port. 2014;27(4):480-8.
2. Nasser N. Melanoma cutâneo - estudo epidemiológico de 30 anos em cidade do Sul do Brasil, de 1980-2009. An Bras Dermatol. 2011;86(5):932-41.
3. Konrad P, Fabris MR, Melao S, Blanco LFO. Perfil epidemiológico e histopatológico dos casos de melanoma cutâneo primário diagnosticados em Criciúma no período entre 2005 e 2007. An Bras Dermatol. 2011;86(3):457-61.
4. Ríos L, Nagore E, López JL, Redondo P, Martí RM, Fernández-de-Misa R, et al. Registro nacional de melanoma cutáneo. Características del tumor en el momento del diagnóstico:15 años de experiência. Actas Dermosifiliogr. 2013;104(9):789-99.
5. Battisti R, Nunes DH, Lebsa-Weber A, Schweitzer LC, Sgrott I. Avaliação do perfil epidemiológico e da mortalidade dos pacientes com diagnóstico de melanoma cutâneo primário no município de Florianópolis - SC, Brasil. An Bras Dermatol. 2009;84(4):335-42.
6. Chiba FB, Delfino ACG, Schettini APM, Chirano CA, Damasceno SAS. Perfil clinicoepidemiológico dos melanomas cutâneos em duas instituições de referência na cidade de Manaus, Brasil. An Bras Dermatol. 2011;86(6):1239-41.
7. Brasil. Ministério da Saúde. Portaria nº 357, de 8 de Abril de 2013. Aprova as Diretrizes Diagnósticas e Terapêuticas do Melanoma Maligno Cutâneo. Diário Oficial [da] República Federativa do Brasil. 2013 abr. 08 [acesso em 2015 maio 19]. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0357_08_04_2013.html
8. Bonfá R, Bonamigo RR, Bonfá R, Duro KM, Furian RD, Zelmanowicz AM. A precocidade diagnóstica do melanoma cutâneo: uma observação no sul do Brasil. An Bras Dermatol. 2011;86(2):215-21.
9. Criado PR, Vasconcellos C, Sittart JAS, Valente NYS, Moura BPS, Barbosa GL. Melanoma maligno cutâneo primário: estudo retrospectivo de 1963 a 1997 no Hospital do Servidor Público Estadual de São Paulo. Rev Assoc Med Bras. 1999;45(2):157-62.
10. Ferrari Júnior NM, Muller H, Ribeiro M, Maia M, Sanches Júnior JA. Cutaneous melanoma: descriptive epidemiological study. Sao Paulo Med J. 2008;126(1):41-7.
11. Dimatos DC, Duarte FO, Machado RS, Vieira JV, Vasconcellos ZAA, Bins-Ely J, Neves RD. Melanoma cutâneo no Brasil. Arquivos Catarinenses de Medicina. 2009;38(01):14-19.
12. Purim KSM, Sandri CO, Pinto NT, Sousa RHS, Maluf EPC. Perfil de Casos de Melanoma em um Hospital Universitário, 2003 a 2007. Revista Brasileira de Cancerologia 2013;59(2):193-199.
13. Pinheiro AMC, Friedman H, Cabral ALSV, Rodrigues HA. Melanoma cutâneo: características clínicas, epidemiológicas e histopatológicas no Hospital Universitário de Brasília entre janeiro de 1994 e abril de 1999. An Bras Dermatol. 2003;78(2):179-86.
14. Salvio AG, Assumpção Júnior A, Segalla JGM, Panfilo BL, Nicolini HR, Didone R. Experiência de um ano de modelo de programa de prevenção contínua do melanoma na cidade de Jaú-SP. An Bras Dermatol. 2011;86(4):669-74.
15. Schaffer JV, Rigel DS, Kopf AW, Bolognia JL. Cutaneous melanoma - past, present and future. J Am Acad Dermatol. 2004;51(1 Suppl):S65-9.
16. Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Sammarco E, Delfino M. Epiluminescence Microscopy for the Diagnosis of Doubtful Melanocytic skin Lesions. Arch Dermatol. 1998;134:1563-70.
17. Vilanova CMA, Lages RB, Ribeiro SM, Almeida IP, Santos LG, Vieira SC. Perfil epidemiológico e histopatológico do melanoma cutâneo em um centro do nordeste brasileiro de 2000 a 2010. An Bras Dermatol. 2013;88(4):553-62.
18. Callender GG, Egger ME, Burton AL, Scoggins CR, Ross MI, Stromberg AJ, et al. 30. Prognostic implications of anatomic location of primary cutaneous melanoma of 1 mm or thicker. Am J Surg. 2011;202:659-64.
19. Venegas LFP, Flores C, Blacher GG, Daudt AW, Cerski CTS. Melanoma maligno cutâneo no Rio Grande do Sul: estudo de 101 casos. Rev Ass Med Brasil.1992;38:122-6.
20. Hampe SV. Estudo da precocidade diagnóstica dos melanomas cutâneos primários em Porto Alegre, por análise de imagem computadorizada [Tese]. Porto Alegre (RS): Universidade Federal do Rio Grande do Sul; 1997. 132 p.
21. Lapa MS, Guedes KF, Schslch FO, Landman G. Melanomas malignos cutâneos tratados no Hospital do Câncer de São Paulo. Estudo retrospectivo para avaliação de distribuição, fatores prognósticos e sobrevida. An Bras Dermatol. 2002;77:313-20.
22. Brandão FV, Pereira AFJR, Gontijo B, Bittencourt FV. Aspectos epidemiológicos do melanoma em serviço de dermatologia de hospital universitário em um período de 20 anos. An Bras Dermatol. 2013;88(3):348-57.
This study was performed at Instituto Lauro de Souza Lima - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}