


Célia Luiza Petersen Vitello Kalil1; Renata Hübner Frainer2; Letícia Santos Dexheimer2; Renata Elise Tonoli3; Ana Letícia Boff4
Keywords: ACNE VULGARIS; CICATRIX; COMBINED MODALITY THERAPY; ESTHETICS
Acne vulgaris is one of the most common skin diseases. After the active inflammatory phase, most patients develop atrophic scars. 1-4 Acne scars are an aesthetic and psychological problem. Studies have confirmed their psychosocial impact, demonstrating a higher incidence of disorders, including introverted personality and depression in patients with severe acne scars.5 To date, there is no standard treatment. Several options have been described with diverse clinical outcomes and complications, such as various surgical techniques, dermabrasion, fractional ablative and non-ablative lasers, chemical peels, resurfacing, autologous fat transplant, and cutaneous fillers. 2
More recently, percutaneous collagen induction therapy (PCIT) using plastic rollers equipped with microneedles, was introduced in Europe, with very good results. Desmond Fernandes was the first to call this technique microneedling or PCIT, in 1993 in France. 1, 4 Different brands of such single-use rollers with needles, varying in number (from 192 to 1074) and length (from 0.25 mm to 3 mm) 0.1 mm in diameter, have now been commercialized worldwide.
The area to be treated should receive firm pressure from the device, and the needles must penetrate up to the dermis. Each pass of the needled device produces at least 16 micropunctures / cm2. The device must roll in forwards and backwards movements, in different directions, 10 to 20 times. 1-6 The microinjuries in the papillary dermis create a confluent zone of superficial bleeding that acts as a powerful stimulus to trigger the healing process, releasing various growth factors, which in turn stimulate fibroblast proliferation and the synthesis of collagen types I and III. With the conversion of collagen from type III into type I, there is a contraction in the collagen network, which reduces the laxity of the skin and softens rhytids and scars.
Newly formed fibroblasts and capillaries migrate through the punctured tissue of the treatment area. The process results in the formation of new tissue that "fills" the atrophic scars and induces repigmentation by improving the blood supply. The microneedling therefore results in neocollagenesis and neoangiogenesis. The tissue remodeling continues for months after the procedure. 2,3,6
There are studies that demonstrate the beneficial effect of topical application of growth factors such as EGF (epidermal growth factor), IGF (insulin-like growth factor) and TGF-β3 (transforming growth factor), contributing to the formation of granulation tissue, decreased skin pigmentation due to the inflammatory process, and maturation of collagen. 7,8
Previous treatments with the microneedling technique used to treat acne scars have demonstrated its effectiveness. 1-6 The advantages of microneedling are: rapid implementation, low cost, and easy approach in areas of difficult access.
The objective of this prospective, single-center study was to evaluate the improvement of atrophic acne scars in the face after treatment with the microneedling technique, followed by topical application of a gel containing growth factors.
The study was approved by the Study and Research Center (CEP) of the Hospital Irmandade Santa Casa de Misericórdia de Porto Alegre, with patients having completed a Free and Informed Term of Consent form. It took place between January 2012 and December 2014. The authors selected 10 patients (6 women and 4 men) aged between 20 and 40 years, who sought out the dermatology ambulatory of the hospital and met the study's criteria. All patients had moderate to severe atrophic acne scars on the face and underwent three sessions, with intervals varying from one to two months. Patient follow-up was one year in duration.
The evaluation was carried out through the histological study of treated skin samples and digital photographs.
Biopsies were taken before the treatment and 30 days after the last session. The samples were stained with Hematoxylineosin and Picrosirius for the evaluation of collagen fibers.
Patients were photographed prior to and subsequent to the procedures, with a commercial digital camera and a digital camera equipped with the Anthera 3D® system (Miravex, Dublin, Ireland), which provides three-dimensional analysis of the skin through the image captured from four elements (color, relief, melanin, and hemoglobin), allowing pre- and posttreatment comparisons.
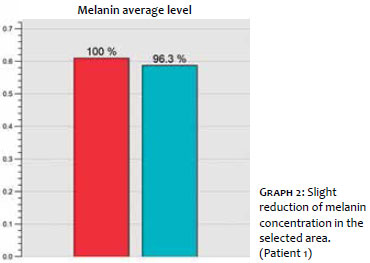
This system analyzes the variables enumerated above at precisely the same location, before and after the treatment, generating reports through graphs. Taking into consideration melanin, for example, it is possible to assess the following variables, based on the graph:
(1) average value: concentration of melanin in the selected area;
(2) melanin variation: distribution of pigment in the selected area. The smaller the variation, the more homogeneous the distribution of melanin in the area;
(3) relative variation (of the melanin in the target area): divides the values of (1) by those depicted in Graph 2, normalizing the distribution of pigment in the selected area, regardless of skin type.
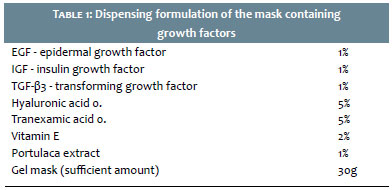
After cleansing the face, the topical anesthetic Dermomax® (Laboratório Aché, São Paulo Brazil) was applied and left on the skin for 60 minutes. Some patients required anesthetic blockage with lidocaine. After the removal of the anesthetic, the microneedling procedure started with a Dr. Roller® sterile device (MTO, Porto Alegre, RS, Brazil) containing 192 needles of 2.0 mm. The passes with the roller were directed horizontally, vertically, and obliquely, as if a compass rose were being drawn, with ten repetitions in each direction. There was a minimum exudation of blood during the procedure, which disappeared after cleansing with sterile saline solution, leaving an erythema and edema. A mask (dispensing pharmacy Dermogral, Porto Alegre, RS, Brazil) containing the following formula was applied soon after. (Table 1)
The purpose of using such active principles delivered via a gel mask after the microneedling was to increase hydration, stimulate fibroblasts, improve healing and cause anti-inflammatory action.
Post-operative
All patients were able to return to their normal activities the day after the procedure. Momentary erythema and edema could be observed on the skin immediately after the treatment. There were no complaints of post-operative pain . Physical sunscreen of SPF 30 was provided for use during the subsequent days.
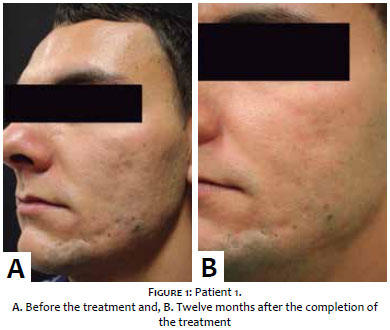
Eight patients completed the study. During the photographic analysis, it was possible to observe global improvement of the skin's appearance and a slight improvement of the extensible atrophic scars. Ice pick type atrophic scars (not extensible) did not improve with the procedure. Comparative photographs (Figure 1) show a patient with improvement of extensible depressed scars.
Anthera system
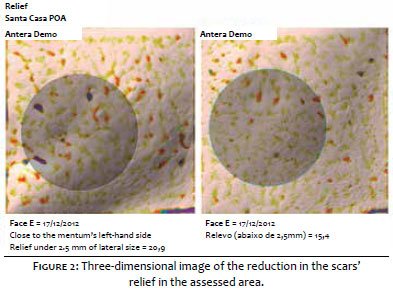
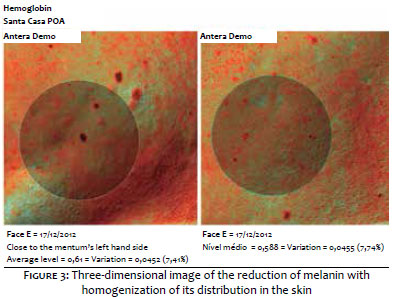
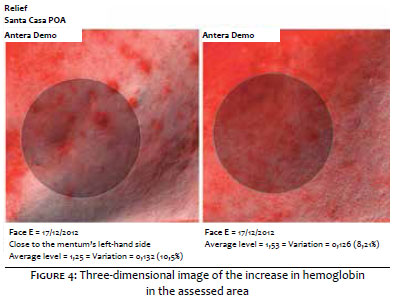
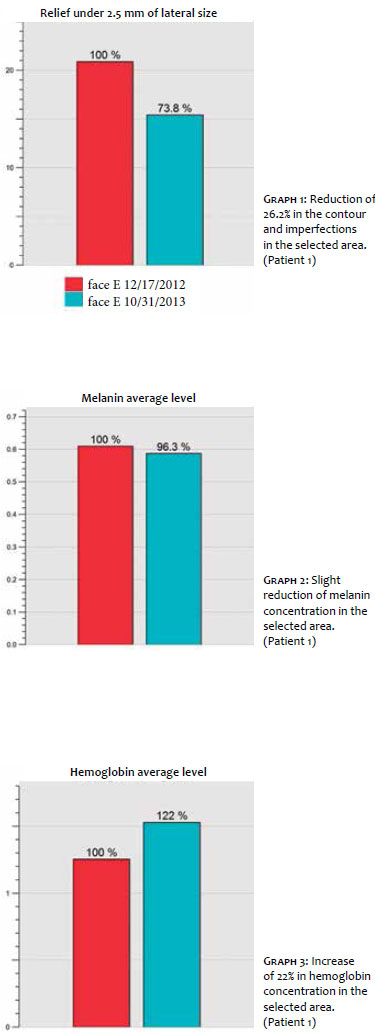
Seven patients had a reduction in the relief of the scars in the area assessed (Figure 2), seven had a reduction of melanin with homogenization of its distribution in the skin (Figure 3), and seven had an increase in hemoglobin in the study area (Figure 4), with the appearance having varied among the eight selected patients.
The analysis of photographs by the Anthera 3D system demonstrated an improvement in the skin's texture, a small reduction in the concentration of melanin, and an increase in hemoglobin concentration in the areas selected. (Graphs 1 to 3)
Pathological examination
The pathological evaluation was performed prior to the procedure in ten cases and in eight cases after the treatment.
The histological findings are described in Table 1, with the following items having been evaluated before and after the microneedling: periadnexal fibrosis, cicatricial fibrosis (with horizontalized collagen), perivascular infiltrate, perivascular edema, thickened collagen presence in the deep dermis in the Picrosirius staining, and thinning of the epidermis after the treatment.
In a study that analyzed 480 patients undergoing PCIT aimed at improving scars and wrinkles, Aust et al. 4 identified increased collagen in the pathology of patients after applying the treatment, with the samples having been submitted to the collagen-specific Van Gieson staining method.
In a study that showed the improvement of photodamage with the induction of collagen production by PCIT, Fernandes et al. 6 identified an absence of thinning of the epidermis after the application of the treatment. This finding seems to be an advance regarding the other treatments, which mostly promote epidermal thinning, as they are more invasive and lead to greater rupture of the basal layer.
In an experimental study, Emerson Vasconcelos et al. 9 established the correlation between the length of the cylinder's needles used in the microneedling procedure and the depth of the injury inflicted. Microscopic examination immediately after the procedure revealed vascular ectasia and extravasation of red blood cells, affecting the papillary dermis with 0.5 mm long needles, and reaching the reticular dermis with 2.5 mm long needles. Thus, microneedling can have a wide range of clinical indications, depending on the depth reached.
In the present study, after the Picrosirius staining (also a collagen-specific staining method), there was no difference in the collagen production after analyzing the deep dermis, the part of the skin's topography where the treatment reaches its maximum effect. In cases where a biopsy was carried out prior to the treatment, it was possible to observe thicker collagen (Picrosirius) in five of them; where patients were biopsied after the treatment, it was possible to identify thicker collagen in six of them. It was possible to observe that the Picrosirius also colored the collagen more intensely in cases in which more fibrosis secondary to acne scars was identified using hematoxylin and eosin staining (HE). Likewise, there was no difference in the lymphocyte infiltration in the edema or in the thickness of the epidermis before and after treatment, results that can be explained by the small size of the evaluated sample. Also, it was noted that in some cases, the epidermis evidenced thinning and flattening of the interpapillary cones after PCIT, a finding that counters the existing literature.
The studied patients achieved an overall improvement in skin texture and a slight improvement of atrophic scars, corroborating the findings found in the study conducted by Imran Majid, 5 in which 36 of the 37 patients showed a similar response to PCIT.
The authors of the present study believe that the increase in the hemoglobin visualized by the Anthera system is due to the increased vascularization promoted by the initial tissular injury, which is perpetuated over time and provides neocollagenesis.
Ice pick type atrophic scars showed no improvement with the procedure.
Long-term clinical analysis, associated with a pathological study, could demonstrate delayed effects of this procedure on acne scars.
1. Percutaneous Collagen Induction with Dermaroller TM for Management of Atrophic Acne Scars in 31 Thai Patients. Asian Journal of Aesthetic Medicine. 2009;2(1):1-13.
2. Leheta T, Tawdy A. Percutaneous Collagen Induction Versus Full-Concentration Trichloroacetic Acid in the Treatment of Atrophic Acne Scars. Dermatol Surg. 2011;37(2):207-16.
3. Liebl H, Kloth LC. Skin Cell Proliferation stimulated by microneedles. J Am Coll Wound Spec. 2012;4(1):2-6.
4. Aust M, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous Collagen Induction Therapy: an alternative Treatment for Scars, Wrinkles, and Skin Laxity. Plast Reconstr Surg. 2008;121(4):1421-9.
5. Majid I. Microneeddling therapy in Atrophic facial scars: an objective assessment. J Cutan Aesthet Surg. 2009;21(1):26-30.
6. Fernandes D, Signorini M. Combating photoaging with percutaneous collagen induction. Clin Dermatol. 2008;26(2):192-9.
7. Spyrou GE, Naylor IL. The Effect of Basic Fibroblast Growth Factor on Scarring. Br J Plast Surg. 2002;55(4):275-82.
8. Akita S, Akino K, Imaizumi T, Hirano A. Basic Fibroblast Growth Factor Accelerates and Improves Second-Degree Burn Wound Healing. Wound Repair Regen. 2008;16(5):635-41.
9. Lima EVA, Lima MA, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol. 2013;5(2):110¬4.
This study was performed at the Irmandade da Santa Casa de Misericórdia de Porto Alegre - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}