


Sandra Tagliolatto1; Oriete Gerin Leite2
Keywords: REJUVENATION; LIPOLYSIS; COLAGEN; NECK; LASERS
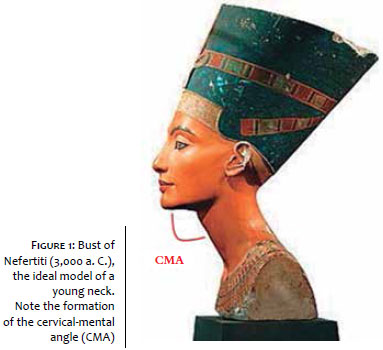
Karlin and Ellenbogen established five visual criteria for the evaluation of the neck and for categorizing its appearance as young looking: a well-delimited mandibular border, presence of sub-hyoid depression, visible prominence of the thyroid cartilage and of the anterior border of the sternocleidomastoid muscle, and a cervical-mental angle (CMA) of between 105º and 120º 1 (Figure 1).
Among the various treatments for the aging cervical region, aimed at restoring the mentioned aesthetic aspects, liposuction under tumescent anesthesia is considered the most effective and minimally invasive procedure due to the fact that it can remove the accumulated fat in the submental region and contribute to the mitigation of local cutaneous sagging. 2 The association of laserlipolysis during the same operative event improves the final result of traditional liposuction, offering even greater improvement in the contour of the neck, due to its action in stimulating the production of collagen. 3-5
Laserlipolysis has been used since the '90s with good results in the treatment of localized fat and body contour definition. With the development of lasers, it has become consistent and effective, with good tolerance and a good safety profile. 6
Several scientific studies carried out in the last decade have shown advantages over surgical methods and traditional liposuction. In addition to the double benefit of subcutaneous fat removal and the remodeling of collagen fibers - clinically evidenced by the skin tightening effect - laserlipolysis provides a shorter recovery time, greater convenience to the patient, and lower post-operative complication rates (hematoma, seroma, asymmetries etc). 7-9
Some reports have shown good results using laserlipolysis in isolation, without the traditional liposuction. However, current studies indicate that isolated laserlipolysis can only be used to treat maximum volumes of up to 100cm3, which makes this technology useful most often in association with local aspiration. 9, 10
In order to perform the laserlipolysis procedure in the cervical region, knowledge of the local anatomy is crucial and will assist both in the appropriate selection of suitable patients and in the planning of the treatment. 11, 12
Knowledge of cervical anatomy and its variations caused by the aging process enables greater precision in the treatment of the aging neck, contributing to the improvement of the results obtained, as well as decreasing the incidence of post-operative complications. 2
Platysma muscle
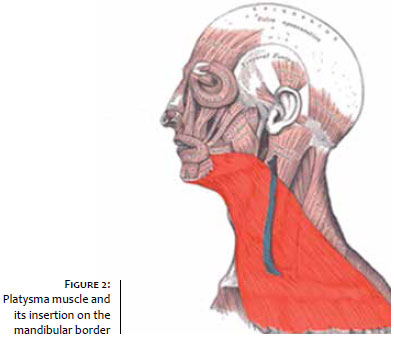
The platysma muscle emerges inferiorly in the cervical thoracic fascia, inserts superiorly to the angle of the oral depressor, risorius and mentonian muscles, and also intermittently in the mandible (Figure 2). 13
Liposuction of the cervical region aims at removing the pre-platysmal adipose tissue, which covers the platysma muscle. 13 The aging of this muscle can be responsible for the formation of the so-called platysmal bands, which negatively alters the aesthetic appearance of the neck, for it contributes to the increase of the CMA, and may also directly impact the sagging of the region (muscle sagging). 14
In the treatment of the aging cervical region, it is therefore necessary to combine therapeutic methods: in addition to the use of techniques for the removal of local fat and cutaneous retraction, surgical techniques of plication of the platysma or the use of botulinum toxin can be associated with treatment of local muscle changes. 15, 16
The platysma muscle receives innervation from the cervical branch of the facial nerve, which in turn acts on the depressor musculature of the lower lip. 13
Marginal mandibular branch of the facial nerve
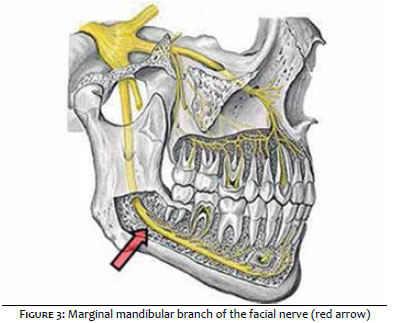
The marginal mandibular branch of the facial nerve runs deeply to the platysma, along the mandible's body (in 80% of cases), or 1 to 2 cm below the mandible (in roughly 20% of cases). 2
This branch surfaces in the anterior border of the masseter muscle and is located anteriorly to the region where the facial artery crosses the mandible (Figure 3). 17, 18
There are no reports of transection or permanent paralysis of the marginal mandibular nerve resulting from liposuction with tumescent anesthesia; however neurapraxia resulting from the temporary interruption of the conduction of nerve impulses and motor function can occur and is a consequence of trauma to the nerve fibers without nerve rupture. 18
In the present study, with over 100 patients, there were no cases of permanent paralysis. There were only two reports of neurapraxia, both with spontaneous resolution in up to four weeks, which is aligned with the literature. There are descriptions of neurapraxia of the marginal mandibular nerve during a period of four to six weeks; though there are references of permanence for up to 12 months. 19
Submandibular salivary glands
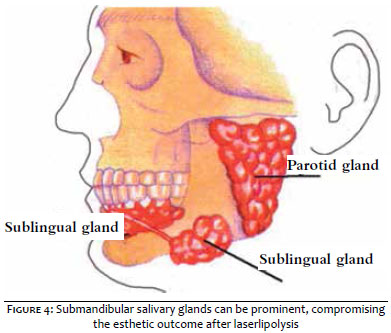
Salivary glands are present in the lower region of the mandibular midline. If prominent submandibular glands become visible after liposuction of the neck, surgical procedures such as resection of glands or other techniques, are required to resolve the aesthetic problem. As a result, patients need to be consulted in regards to this issue (Figure 4). 2, 12
Hyoid bone
The CMA may be altered not only due to the accumulation of fat in the submental area or sagging of the platysma muscle, but also due to the position of the hyoid bone in relation to the mandible. 16
It is generally located roughly at the C3 and C4 level, however in some patients the hyoid bone can be positioned lower, increasing the CMA. This is therefore an anatomical factor that must be taken into account when selecting a patient for the laserlipolysis procedure, since the laser will obviously be ineffective in these patients. 14
In brief, during the clinical examination, the CMA, the submental adiposity accessible to liposuction, the location of the hyoid bone, and the quality of the cervical region's skin must be evaluated, analyzing the degree of photodamage and skin elasticity, as well as observing if there is muscle sagging and/or if there is a presence of platysmal bands and, finally, to attempt to palpate the submandibular glands.
Based on the mentioned clinical findings, it is advisable to discuss the laserlipolysis procedure (with or without liposuction) with the patient in advance, as well as the possible necessity of association with other treatments to achieve the best results in the treatment of the aging cervical region. For example, there may be a need to carry out fractional resurfacing in order to improve the quality of more severely photodamaged skin, or to apply botulinum toxin to mitigate platysmal bands, and even to perform liposuction in another region or even conduct a platysmaplasty. 19
In addition to being attentive in the selection of the patient, a meticulous anamnesis is necessary during the consultation, with an aim at searching for comorbidities or the use of medications that could interfere negatively during or after surgery. It is important to investigate the use of supplements and vitamins with anticoagulant properties, such as ginkgo biloba and vitamin E, among others, which may lead to an increased risk of post-operative complications. 20
It is important to investigate the use of medications that interfere with the metabolism of lidocaine (which is metabolized by the cytochrome P450), even though the anesthetic amount used to carry out the laserlipolysis in the cervical region is small. 21 Allergy to medicines should also be investigated, as well as other complications in previous surgical procedures. 20
In addition to the clinical evaluation, laboratory tests such as coagulogram, serology of hepatitis B, C, and HIV should be requested pre-operatively. Some authors also suggest cardiological evaluation, in the case of patients over 60 years of age and/or with a history of heart disease. 2
Laserlipolysis combined or not with liposuction and performed under tumescent anesthesia, has few contraindications, but those include pregnancy, heart and circulatory disease, and severe coagulation disorders. Although they are not absolute contraindications, greater attention is important in patients who have a history of bleeding, embolism (fatty or thrombotic), and diabetes mellitus. 22
It is necessary to obtain a signed consent form prior to the procedure and provide pre- and post-operative instructions in writing, as follows:
Usual medications, such as antihypertensive and antiglycemic, can and should be taken on the day of the laserlipolysis.
It is also recommended that the patient be instructed to initiate the use of prophylactic antibiotics (cephalosporin), which must be prescribed one day before the procedure, to eat normally, to wear clothes that are easy to put on and take off after the procedure, and to be attentive to the need of being accompanied on the day of the treatment. 2
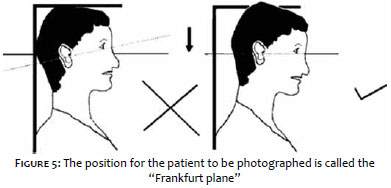
It is crucial to perform photographic records of the patient (frontally and laterally) prior to the laserlipolysis. The photographs must allow for the evaluation the CMA, the submandibular fat and any detail in the anatomy of the neck before and after the procedure.
The ideal position of the patient at the time the photographs are taken is called the Frankfurt plane, which is achieved by tracing an imaginary line from the patient's external ear canal to the inferior channel of the orbicularis rhyme, in anatomical position, with a straight gaze towards the horizon (Figure 5). 18, 23
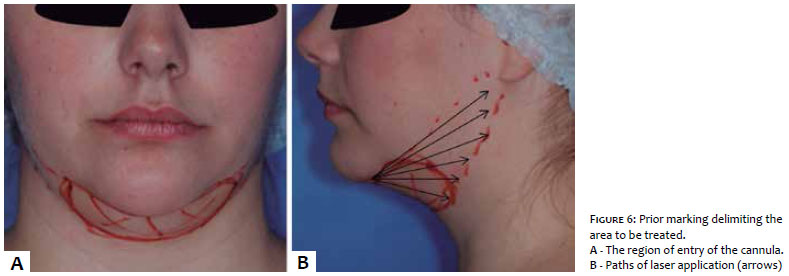
The patient's neck is marked in order to delineate the area to be treated, which includes the submental fat, the lower border of the treated area, the anterior border of the sternocleidomastoid muscle, as well as the mandible's upper (if treated) and lower borders (Figure 6). 2
The entry points can also be marked at this time: the first (and often only) entry point for the cannula is located in the submentum, at approximately 0.5 cm from the posterior border of the mandible. Other entry sites (for the lateral suction, if necessary) are marked on the lateral region of the neck (in the anterior border of the sternocleidomastoid muscle, below the earlobe). 16
It can be helpful to mark the anterior border of the masseter muscle, where the marginal mandibular nerve surfaces. With this, the region to be treated is highlighted during the surgery, helping to prevent some kind of trauma during the procedure. 12
The operating table is prepped with the materials required for preparing the anesthetic solution, as well as with syringes used for injecting it and cannulas. On the table must also be the cannulas for the aspiration of the local fat, scalpel blade and handle (for carrying out the entry orifice for the injection cannulas, laser and, if applicable, the suction cannulas), gauze and compresses.
In the operating room, in addition to the surgical table, is the laser platform with its fibers, monitoring devices (such as pulse oximeter) and emergency equipment.
Before the start of, during, and immediately after surgery, it is prudent to carry out the assessment of vital signs, as well as the measurement of blood pressure and heart rate.
If a sedative is given, bear in mind that it can affect breathing and induce hypoxia and therefore breathing should be monitored and a pulse oximeter should be used. 24
The Klein's tumescent anesthesia without any sedation, was used in the authors procedures. This solution is composed of 1,000 ml of saline, 50 to 100 ml of 1% lidocaine, 1 ml epinephrine 1:1,000 and 12.5 ml of 8.4% sodium bicarbonate. 25
Assuming that the patient is not using any medication that interferes with the metabolism of lidocaine, varying doses of this solution (35 to 55 mg /kg) can be used safely, however this is usually not a problem when the neck region is treated, given the small amount of anesthetic solution (300-500 ml) used to achieve proper tumescence. 26
After performing the anesthesia, there must be a waiting period of 20 to 30 minutes, after which the passage of the 1 mm microcannula containing the laser fiber in the subcutaneous plane is started in slow movements, in a fan pattern, creating tunnels of thermal damage in the adipocytes. 3
The authors point out that the laser must be passed slowly in the subcutaneous, at a speed of 5-10 cm/s, in order to allow its interaction with the target area to take place. On the other hand, the laser should never stop once activated, due to the risk of burns. 6, 7
The laser pass' end point can be detected by monitoring several parameters. The perception of local heat and the "softening" of the subcutaneous region during laser passage are crucial. The procedure can be guided by the accumulated energy values on the device's panel, and temperature monitoring by external or internal thermometers, coupled to the tip of some laser devices. 2, 5, 6
In their practice, the authors of the present article use the 924nm/975nm diode laser device (SlimLipo, Palomar, USA), with two wavelengths - one specific for liquefying the adipose tissue (924nm) and another for skin retraction, due to its action on the collagen and elastic fibers at the level of the deep adjacent dermis (975nm). 27, 28
This device does not allow for the taking of the internal temperature, however the authors adopted the use of an external laser digital thermometer in the study's protocol, for assistance during the treatment. An external temperature of around 40º C is sought during the procedure, since in most cases this leads to good aesthetic results without tissue damage.
The use of devices specific to laserlipolysis requires attention during surgery, regarding the energy emitted by the laser per region - called "accumulated energy" - in order to promote a better aesthetic result based on the remodeling of the fibrous connective tissue. 29
The control of the accumulated energy is an essential safety parameter aimed at reducing the risk of side effects such as necrosis, prolonged erythema, and dyschromia. 5
Once the end point of the laser passage is reached, the aspiration of "molten fat" can be performed or not, depending on the volume treated. Alternatively, the manual "milking" can be performed without the cannula, in the case of smaller volumes.
While performing the liposuction, it is necessary to use the appropriate cannula for the cervical region in order to avoid unnecessary damage. The delicate passage of the cannula under mild negative pressure is sufficient to remove the liquefied fat. Technical care, such as attention to the region of the approximate path of the marginal mandibular branch of the facial nerve, is necessary in the execution of suction. For this, it is necessary to avoid the lateral rotation of the head (with the risk of forcing the nerve into a more superficial position, 2 to 3 cm below the mandible) and to use the hand as a guide when performing the surgery. 12, 16, 18, 19
At the end of the procedure, local compression is used (occlusive dressing and a compressive neck garment) in order to facilitate the remodeling of the skin, minimizing the risk of folds, preventing bruising and/or seroma formation, and improving absorption and drainage of the remaining tumescent fluid. 22
Post-operative care
Regarding the compressive garment, it should be used continuously (24 hours a day, removing only for bathing) during the first two days, and for 2 to 4 hours a day in the following two weeks. The occlusive dressing should remain in place for the first 18 hours, when the greatest drainage of remaining liquid takes place. 30
It is recommended that the patient avoid physical exercise for 7 days, and some authors suggest that attention must be paid regarding the temperature of the water used when bathing, and the use of ice directly on the skin, in order to avoid damage.
Although complications are rare, contact numbers should always be provided to patients in the event of any undesirable side effect, which should always be assessed. 2, 30
The patient must return periodically in order to monitor the progressive improvement of the region: resolution of the edema, formation of collagen, and retraction of the skin, all of which occur within a few months - up until 18 months after the date of the procedure, according to some authors. 16
Discussion of the literature: efficacy and safety
Laserlipolysis is a minimally invasive therapeutic modality that is being used at an increasing rate to treat localized fat, and for the rejuvenation and definition of the contour of the body and face. 31 Since the first studies were published in the 90's, several reports have been published every year, with different laser types, wavelengths, and fat and water absorption coefficients. 3-12
The most frequently described lasers are the 920nm, 924/975nm and 980nm diode lasers, as well as the 1,064nm, 1,319nm, 1,320nm, 1,440nm and 1,444nm Nd:YAG lasers. Despite the different wavelengths, all laserlipolysis systems work on the principle of selective photothermolysis, i.e. action of heat in specific tissues, such as fat and collagen. 6, 31
The laser releases energy, which is retained in the form of heat in the subcutaneous tissue in contact with the optical fiber. The heat captured by the adipocytes can lead to the rupture of cell membranes, with the release of intracellular lipases, promoting liquefaction of the adipose tissue, which facilitates liposuction with less trauma and bleeding. 32
When absorbing the heat, collagen fibers of the adjacent dermis undergo denaturation, stimulating the remodeling and contraction of collagen, and promoting neocollagenesis. Histological studies have shown that heat destroys adipocytes via the creation of small pores in the membranes of these cells. 33
In addition to lipolysis, coagulation of blood vessels and sweat glands occurs, and the reorganization of collagen and elastic fibers. Clinically, these findings correlate to the skin tightening effect and to less bleeding during and after surgery. 7, 33
While there is still a search for better parameters, laserlipolysis - with or without aspiration - has been used in the treatment of submental adiposity for two decades with good results (Figure 7). 11, 12
In 2002, Goldman et al. published a case study series with 1,734 patients who underwent laserlipolysis in various body sites, including the submentum, with low blood loss and ecchymosis, little post-operative discomfort, and fast recovery, in addition to a low complication rate. 34 In 2006, the same author published a retrospective with 82 patients who underwent laserlipolysis of the submental region with and without aspiration. In addition to an efficacy comparable to that of conventional liposuction, it was possible to observe clinical and histological retraction of the skin, and collagen neoformation. 7
The use of tumescent anesthesia for liposuction allows for the safe removal of fat, with minimal blood loss and little post-operative pain. There are no reports of mortality or even significant morbidity associated with liposuction under tumescent anesthesia. 35
Hanke et al. studied 15,336 patients and 44,014 body sites treated with liposuction using tumescent anesthesia, and did not find cases of death or serious complications requiring transfer to a hospital. 36 Housman et al. reported 66,570 liposuction procedures performed by dermatologic surgeons from 1994 to 2000, with an absence of reports of deaths. Adverse events requiring hospitalization occurred at a rate of 0.68 per 1,000 cases, with the use of sedatives described as an identified risk factor. 37
The use of the ideal accumulated energy maximizes the effects of the laserlipolysis, which are the removal of subcutaneous fat and the retraction of the skin. Reynaud et al. reviewed the values of the accumulated energy used in the various studies published up until 2009 and detected a progressive increase of the parameters over time and associated with better clinical outcomes. In their series of 534 procedures, 22 patients underwent laserlipolysis in the submentum with 980nm diode laser at 6W of potency. The average accumulated energy in the submental region was 11,700J. 8
More recently Sarnoff evaluated the use of 1,440nm Nd:YAG, without aspiration, in the treatment of the cervical contour in 24 patients, having employed an average accumulated energy 1,205J per 5x5cm. Improvement of 79% was obtained in CMA values and in the overall aesthetic score. 38
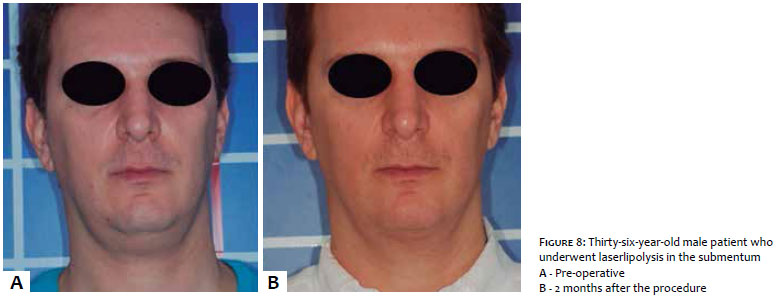
In the experience of the authors of the present article, an accumulated energy of 5,000J per 10cm2 area is close to ideal as a progressive and persistent retraction of the skin can be observed at this level, with a reduction of side effects such as ecchymosis, prolonged erythema, excessive bleeding, or the formation of dimples in the skin (Figures 8 and 9). 6-8, 12, 31, 38
It is known that low energy levels cause reversible swelling of adipocytes and that high energy levels are responsible for the lysis of adipocytes and significant improvement of the results. Nevertheless, high energies increase the risk of thermal injury to the skin. 11, 12
Kim and Geronemus found a volumetric reduction of 25% in the submental fat, measured by MRI, after three months of laser application in 5 patients. In a total of 29 patients, they observed a positive correlation between the accumulated energy and the reduction in the volume of the treated area. 3
Some studies have begun to emerge that try to correlate the measurement of the external temperature with the safety and effectiveness of laserlipolysis. In 2012, Alexiades-Armenakas achieved good results with the use of 1,064nm and 1,319nm lasers, either isolated or in combination, in the treatment of submental adiposity and sagginess. The internal temperature of the target tissue was 45ºC to 48ºC. Most authors consider external temperatures around 40ºC as safe and effective. 12
Apparently, complication rates of laserlipolysis are lower when compared to that of traditional liposuction. Sarnoff has not recorded cases of seroma, infection, damage to the mandibular nerve, dyschromia or hematomas. 38 After 1,000 consecutive cases of laserlipolysis, Chia et al. described 3 cases of skin burn, 2 of infection, 1 of seroma and 1 of hematoma, clearly related to a learning curve since they occurred in the first 25 cases. In 7.3% of cases retreatment was required due to insufficient improvement. 22
The satisfaction rate with laserlipolysis was assessed in a study by Leclère et al. in 2014. After laserlipolysis in the submentum of 30 patients, it was possible to observe a systematic improvement in the CMA, in the cutaneous retraction, and in the decrease of subcutaneous fat. The procedure was recommended by all patients and was highly satisfactory among evaluators. 39
There is a consensus among authors that the correct patient indication leads to more satisfactory results. Advanced aging, exuberant adiposity, and a high degree of sagging compromise the final result of laserlipolysis. 2, 16
Several additional techniques can be combined with laserlipolysis in order to further improve the neck's appearance, including the treatment of photodamaged skin using fractional CO2 laser, the use of botulinum toxin for mitigating platysmal bands and even surgical procedures performed directly on the platysma. 2
In addition to association with conventional liposuction, laserlipolysis is gaining ground as an adjuvant procedure in the facial mini-lifts. Ramirez et al. obtained esthetical improvement of the neck and submentum in 100% of cases after six months of application of 924/975nm diode laser in conjunction with platysmaplasty in 78 patients. 40
In contrast, some authors studied the isolated application of laserlipolysis for improving facial sagging. Holcomb obtained good results in 478 patients who underwent laserlipolysis to define the contour of and rejuvenate the middle and lower thirds of the face with 1,444nm Nd:YAG. 41 McMenamin treated 40 patients with an aim at promoting the improvement of the facial contour and performing a facelift based on the cutaneous retraction. 42 He obtained good results and higher satisfaction rates as compared to those of the traditional surgery.
The use of laserlipolysis in the treatment of cervical rejuvenation and submental adiposity is a minimally invasive, safe, and effective therapy. The results obtained in several published clinical studies are promising.
The advantages over traditional liposuction are: shorter recovery time, less bleeding, additional effect of cutaneous retraction (or skin tightening) and low retreatment rates.
The different wavelengths and lasers employed appear to have similar effects on the target tissue. Better results are achieved with a greater accumulated energy; nonetheless this fact increases the risk of cutaneous thermal injury. Notwithstanding, reports of burns are rare and are related to the learning curve.
The correct indication of the patient and the association - when necessary - with other rejuvenation methods, such as platysmaplasty, botulinum toxin, and fractional resurfacing, optimizes the final aesthetic result.
The laserlipolysis of the submentum and cervical region is a well-tolerated technique, with high satisfaction rates among patients and physicians, is considered safe and leads to lasting results. Nevertheless, further controlled, randomized, and multicenter studies are still necessary for establishing the technique as the gold standard cervical rejuvenation treatment.
1. Ellenbogen, R., and Karlin, J. V. Visual criteria for success in restoring the youthful neck. Plast Reconstr Surg. 1980;66(6):826-37.
2. Stebbins WG, Hanke CW. Rejuvenation of the neck with liposuction and ancillary techniques. Dermatol Ther. 2011;24(1):28-40.
3. Kim KH, Geronemus RG. Laser lipolysis using a novel 1,064 nm Nd:YAG laser. Dermatol Surg. 2006;32(2):241-8.
4. Sun Y, Wu SF, Yan S, Shi HY, Chen D, Chen Y. Laser lipolysis used to treat localized adiposis: a preliminary report on experience with Asian patients. Aesthetic Plast Surg. 2009;33(5):701-5.
5. Badin AZ, Moraes LM, Gondek L, Chiaratti MG, Canta L. Laser lipolysis: flaccidity under control. Aesthetic Plast Surg. 2002;26(5):335-9.
6. Fakhouri TM; El Tal AK; Abrou AE; Mehregan DA; Barone F. Laser-assisted lipolysis: a review. Dermatol Surg. 2012;38(2):155-69.
7. Goldman A. Submental Nd:Yag laser-assisted liposuction. Lasers Surg Med. 2006;38(3):181-4.
8. Reynaud JP, Skibinski M, Wassmer B, Rochon P, Mordon S. Lipolysis using a 980-nm diode laser: a retrospective analysis of 534 procedures. Aesthetic Plast Surg. 2009;33(1):28-36.
9. Prado A, Andrades P, Danilla S, Leniz P, Castillo P, Gaete F. A prospective, randomized, double-blind, controlled clinical trial comparing laser-assisted lipoplasty with suction-assisted lipoplasty. Plast Reconstr Surg. 2006;118(4):1032-45.
10. Parlette EC. Kaminer ME. Laser-assisted liposuction: here's the skinny. Semin Cutan Med Surg. 2008;27(4):259-63.
11. Gentile RD. Laser-assisted neck-lift: high-tech contouring and tightening. Facial Plast Surg. 2011;27(4):331-45.
12. Alexiades-Armenakas M. Combination laser-assisted liposuction and minimally invasive skin tightening with temperature feedback for treatment of the submentum and neck. Dermatol Surg. 2012;38(6):871-81.
13. Castro CC. The anatomy of the platysma muscle. Plast Reconstr Surg. 1980;66(5):680-3.
14. Prendiville S, Kokoska MS, Hollenbeak CS, et al. A comparative study of surgical techniques on the cervicomental angle in human cadavers. Arch Facial Plast Surg. 2002;4(4):236-42.
15. Kane MA. Nonsurgical treatment of platysmal bands with injection of botulinum toxin A. Plast Reconstr Surg. 1999;103(2):656-63.
16. Rohrich RJ, Rios JL, Smith PD, Gutowski KA. Neck rejuvenation revisited. Plast Reconstr Surg. 2006;118(5):1251-63.
17. Larrabee W, Makielski K. Surgical anatomy of the face. New York, NY: Raven Pres; 1993.
18. Butterwick KJ. Liposuction of the neck. In: DraelosZD, ed. Cosmetic dermatology: products and procedures. Hoboken; New York: Blackwell Publishing; 2010. p. 463-71.
19. Morrison W, Salisbury M, Beckham P, Schaeferle M 3rd, Mladick R, Ersek RA. The minimal facelift: liposuction of the neck and jowls. Aesthetic Plast Surg. 2001;25(2):94-9.
20. Shiffman MA. Warning about herbals in plastic and cosmetic surgery. Plast Reconstr Surg. 2001;108(7):2180-1.
21. Klein J. Cytochrome P450 3A4 metabolism and lidocaine metabolism. In: KleinJ, ed. Tumescent technique: tumescent anesthesia and microcannular liposuction. St. Louis, MO: Mosby, 2000. p. 133.
22. Chia CT, Theodorou SJ. 1,000 consecutive cases of laser-assisted liposuction and suction-assisted lipectomy managed with local anesthesia. Aesthetic Plast Surg. 2012;36(4):795-802.
23. Farkas LG, Sohm P, Kolar JC, Katic MJ, Munro IR. Inclinations of the facial profile: art versus reality. Plast Reconstr Surg. 1985;75(4):509-19.
24. Svedman KJ, Coldiron B, Coleman WP 3rd, Cox SE, Jacob C, Lawrence N, et al. ASDS guidelines of care for tumescent liposuction. Dermatol Surg. 2006;32(5):709-16.
25. Coleman WP 3rd, Glogau RG, Klein JA, et al. Guidelines of care for liposuction. J Am Acad Dermatol. 2001;45(3):438-47.
26. Coleman WP 3rd1, Glogau RG, Klein JA, Moy RL, Narins RS, Chuang TY, et al. Tumescent anesthesia with a lidocaine dose of 55 mg/kg is safe for liposuction. Dermatol Surg. 1996;22(11):921-7.
27. Weiss RA, Beasley K. Laser-assisted liposuction using a novel blend of lipid- and water-selective wavelengths. Lasers Surg Med. 2009;41(10):760-6.
28. Wolfenson M, Roncantti C, Alencar AH, Barros T, Silva Neto JF, Santos Filho FCN. Laserlipolysis: skin tightening and prevention of flabby umbilical region with lipoplasty following security parameters for use of diode laser with double wavelength 924 and 975 nm. Rev Bras Cir Plast. 2011;26(2):259-65.
29. Mordon SR, Wassmer B, Reynaud JP, Zemmouri J. Mathematical modeling of laser lipolysis. Biomed Eng Online. 2008;7:10.
30. Jacob C, Kaminer M. Rejuvenation of the neck using liposuction and other techniques. In: RobinsonJ, HankeC, SiegelD, editors. Surgery of the skin: procedural dermatology. 2nd Edition. Philadelphia, PA: Elsevier Mosby. 2010. p.691-701.
31. McBean JC, Katz BE. Laser Lipolysis: An Update. J Clin Aesthet Dermatol. 2011;4(7):25-34.
32. Goldman A, Geronemus RG, Kim K. Lipoaspiração a laser. Laserlipólise. In: Toledo LS, editor. Lipoplastia. Rio de Janeiro: Di-Livros. 2006. p. 111-21.
33. Badin AZ, Gondek LB, Garcia MJ, Valle LC, Flizikowski FB, Noronha L. Analysis of laser lipolysis effects on human tissue samples obtained from liposuction. Aesthetic Plast Surg. 2005;29(4):281-6
34. Goldman A, Schavelzon DE, Blugerman GS. Laserlipolysis: liposuction with Nd: YAG Laser. Rev Soc Bras Cir Plást. 2002;17(1):17-21.
35. Triana L, Triana C, Barbato C, Zambrano M. Liposuction: 25 years of experience in 26,259 patients using different devices. Aesthet Surg J. 2009;29(6):509-12.
36. Hanke W, Cox SE, Kuznets N, Coleman WP 3rd. Tumescent liposuction report performance measurement initiative: national survey results. Dermatol Surg. 2004;30(7):967-77.
37. Housman TS, Lawrence N, Mellen BG, George MN, Filippo JS, Cerveny KA, et al. The safety of liposuction: results of a national survey. Dermatol Surg. 2000;28(11):971-8.
38. Sarnoff DS. Evaluation of the safety and efficacy of a novel 1440 nm Nd:YAG laser for neck contouring and skin tightening without liposuction. J Drugs Dermatol. 2013;12(12):1382-8.
39. Leclère FM, Moreno-Moraga J, Alcolea JM, Casoli V, Mordon SR, Trelles MA, et al. Laser Assisted Lipolysis for Neck and Submental Remodeling in Rohrich Type I to III Aging Neck: A Prospective Study in 30 Patients. J Cosmet Laser Ther. 2014 Dec;16(6):284-9.
40. Ramirez P, Leibowitz A, Traylor-Knowles M, Taghizadeh F. Short-flap face-lift with 924 nm/975 nm laser lipolysis: a retrospective study of 78 patients. J Cosmet Dermatol. 2014;13(1):22-9.
41. Holcomb JD. Thermally confined micropulsed 1444-nm Nd:YAG interstitial fiber laser in the aging face and neck: an update. Facial Plast Surg Clin North Am. 2014;22(2):217-29.
42. McMenamin P. Laser face-lifts: a new paradigm in face-lift surgery. Facial Plast Surg. 2011;27(4):299-307.
This study was performed at the authors' private practice in Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}