


Elisa de Oliveira Barcaui1; Antonio Carlos Pires Carvalho2; Paulo Marcos Valiante3; Juan Piñeiro-Maceira4; Carlos Baptista Barcaui5
Keywords: CARCINOMA, BASAL CELL; HIDROCYSTOMA; NEOPLASMS; ULTRASONICS
With the aim of improving clinical-dermatological diagnosis, a range of new imaging methods is being developed. Techniques such as dermoscopy, confocal microscopy, optical tomography, and High-Frequency Ultrasound (HFUS) enable real time examination of the skin's surface, assisting the diagnosis, the guiding of surgical procedures, the monitoring of lesions, and follow-up treatments. 1, 2 However, these methods vary considerably regarding their penetration, resolution and applicability. 3
With the aid of these imaging examinations, lesions that are clinically similar but have different behaviors can be better assessed in the pre-operative phase, which leads to the indication of the most appropriate therapeutic approach.
Dermoscopy or superficial confocal microscopy is a diagnostic method that allows for the recognition of morphological structures that are not observable with the naked eye, through the aid of a manual device that associates a magnifying lens and cross-polarized light. It has a great impact on dermatology practice, and in most cases allows for the differentiation of malignant and benign skin lesions, as well as delimiting their extent in the longitudinal and horizontal axes. Nevertheless, it is unable to assess tumor consistency (cystic or solid) and the depth of hypopigmented lesions. 4
Used in dermatology since the 1970s, ultrasonography is based on the reflection of sound waves through the tissues. According to the anatomical structure, vascularization and density, the ultrasonic waves are reflected back to the transducer, which transforms them into a gray scale that is observable on the monitor. 5, 6 Images are obtained through vertical sections, and both penetration and resolution vary according to the frequency. 3 The recent development of devices with frequencies higher than 15 MHz are the origin of the high frequency ultrasound (HFUS) that has enabled the identification of the skin's different layers, structures, and appendages, and thereby considerably increasing the use of ultrasounds in various dermatological conditions. These devices have low penetration and hence excellent resolution for the visualization of superficial structures. 6
In normal skin, the echogenicity of each layer depends on its main component, which in the epidermis, is keratin; in the dermis, the collagen; and in the subcutaneous, the fat lobules. In ultrasound imaging, the epidermis appears as a hyperechoic line, while the dermis appears as a less echogenic hyperechoic band than the epidermis, and the subcutaneous layer appears as hypoechoic, with the presence of hyperechoic fibrous septa inside it. 7
In the case of skin cancer, HFUS allows for the delimiting of the lesion due to the difference in refraction between the tumor area and the perilesional region, also making it possible to measure the dimensions in both the lateral and depth directions. It also enables the study of tumor consistency through its echogenicity. Solid lesions are often hypoechoic, while echogenicity is variable in cystic lesions, depending on the density of its contents. 5, 6
Of all cancers, basal cell carcinoma (BCC) is the most common, representing 75-80% of all skin cancers. Usually found in people over 60 years of age, its incidence has been increasing in young people. BCCs differ in clinical and histological type. Despite the low metastatic power of BCC, local invasions are common. Studies indicate a high rate of recurrence of the lesions located in the face (especially in the eyelid, nose, and ear) and of those previously excised incompletely. As a result, therapeutic measures such as extensive surgical resection are often adopted and can lead to functional and aesthetic problems; differentiating BCC from other diseases that allow more conservative approaches is of fundamental importance.
The hidrocystoma is a benign cystic neoplasia originating from the sweat gland's duct. Histologically, it is classified as eccrine and apocrine. It typically appears as translucent papules located most often on the face and despite their cystic origin are often clinically mistaken for solid masses, especially BCCs. Conservative treatments such as CO2 laser, topical application of 1% atropine or botulinum toxin type A injections have therapeutic success. 8, 9
The authors analyzed two female patients (one with 74 and the other 72 years of age), both with a single lesion located on the left side of the nose, with an average development time of one year. Regarding their past medical history, the first had undergone excision of the lesion in the dorsum of the nose repaired through a rotation flap three years before, with histology indicating a completely excised nodular type BCC. Clinical, dermoscopic and 22MHz HFUS were performed in both cases.
After the completion of pre-operative tests, the patients underwent an excisional biopsy with the material being sent in formaldehyde solution for histological examination. Routine staining with hematoxylin-eosin (HE) was used in the skin lesions and subsequent microscopic analysis was carried out with 40X and 100X magnification.
The patients' selection criteria was the similarity of the lesion's location in individuals with the same skin phototype, in addition to similar clinical pictures and approximate age.
Clinically, the patients had papular, normochromic lesions, devoid of translucent appearance, located on the left side of the nose, suggesting solid tumor masses (Figure 1A and B).
The dermoscopic examination showed similar findings in both cases, with the presence of arboriform telangiectasia (Figure 2A and B).
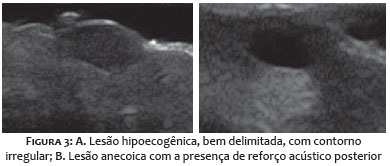
Under HFUS, the first patient revealed an oval, hypoechoic, poorly defined lesion located in the dermis. In the second case, a well-defined anechoic lesion located in the dermis was observed with the presence of posterior acoustic enhancement, indicating cystic appearance and the presence of liquid content (Figure 3 A and B).
In the first case, histology showed basaloid cell nests located in the dermis. In the second case, it revealed a dermal cystic lesion located in the dermis and covered by columnar epithelium. The respective conclusive reports were: nodular type BCC and eccrine hidrocystoma (Figure 4 A and B).
To date, histology is the gold standard for diagnosis and morphological and structural assessments of cutaneous neoplasias. However, new techniques for in vivo diagnosis have been used to accelerate diagnosis and optimize pre-operative evaluation.
Although the defining dermoscopic criteria for diagnosis of BCC (absence of pigmented network associated with the presence of ovoid nests, ulceration, multiple gray-bluish globules, leaf-like structures, radiated areas and/or arboriform telangiectasia) are well established, the hidrocystoma can present dermoscopic structures that simulate these findings, hampering the dermoscopic diagnosis of these two entities. 4
Based on the echogenicity observed through the HFUS, it is possible to distinguish these two types of skin tumors. In BCC, hypoechoic, well-delimited lesions with irregular contours are observed. There is often a presence of hyperechoic spots within. These images are attributed to the presence of corneal cysts, microcalcifications and clusters of apoptotic cells within the tumor mass. 7 A study by Chin et al. using HFUS indicates that hidrocystomas usually have a hyperechoic surface with anechoic content (clear fluid) or hypoechoic center. 10 In the present study, the authors observed delimited lesions, with hyperechoic surfaces, well-defined contours and anechoic content, suggesting cystic content.
HFUS can be considered an excellent method for the evaluation of skin tumors. Unable to assess tumor cellularity, it cannot be used to confirm the diagnosis, nonetheless it enables the performing of a detailed pre-operative study, analyzing the different skin layers and their thicknesses, indicating the tumor's nature (cystic or solid), gauging their size, precise location, and involvement of adjacent structures, all of which are important parameters to guide the therapeutic approach.
1. Mogensen M, Morsy Ha, Thrane L, Jemec GBE. Morphology and epidermal thickness of normal skin imaged by optical coherence tomography. Dermatology. 2008;217(1):14-20.
2. Psaty EL, Halpern AC. Current and emerging technologies in melanoma diagnosis: the state of the art. Clin Dermatol. 2009;27(1):35-45.
3. Ulrich M, Stockfleth E, Roewrt-Huber J, Astner S. Noninvasive diagnostic tools for nonmelanoma skin cancer. Br J Dermatol. 2007;157 Suppl2:56-8.
4. Ferreira CMM, Barcaui C, Piñeiro-Maceira J. Atlas de dermatoscopia aplicação clínica e correlação histopatológica. 2 ed. Rio de Janeiro: Di Livros; 2011.
5. Wortsman X, Wortsman J. Clinical usefulness of variable-frequency ultrasound in localized lesions of the skin. J Am Acad Dermatol. 2010;62(2):247-56.
6. Kleinerman R, Whang TB, Bard RL, Marmur ES. Ultrasound in dermatology: principles and applications. J Am Acad Dermatol. 2012;67(3):478-87.
7. Worstman X. Sonography of facial cutaneous basal cell carcinoma. A first line imaging technique. J Ultrasound Med. 2013;32(4):567-72.
8. Sanz-Sanchez T, Dauden E, Perez-Casas A, Ortiz-del Portillo A, Jones M, García-Díez A. Efficacy and safety of topical atropine in treatment of multiple eccrine hidrocystomas. Arch Dermatol. 2001;137(5);670-1.
9. Woolery-Iloyd H, Rajpara V, Nijhawan RI. Treatment for multiple periorbital eccrine hidrocystoma: botulinumtoxin A. J Drugs Dermatol. 2009;8(1):71-3.
10. Furuta M, Shields CL, Danzing CL, Eagle RC Jr, Shields JA. Ultrasound biomicroscopy of eyelid eccrine hidrocystoma. Can J Ophthalmol. 2007;42(5):750-51.
This study was performed at the Radiology Department of the Universidade Federal do Rio de Janeiro (UFRJ) and at the Dermatology Service of the Universidade Estadual do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}