


Rodolfo Chedid1; Janaina Nagel2; Taynara de Mattos Barreto3; Glaura Tinoco Plata4; Anna Luiza Bento Dutra3; Thales Pereira de Azevedo3,1
Keywords: ECCRINE SPIROADENOMA, BENIGN EPITHELIAL NEOPLASIA, SEBACEOUS GLANDS
Eccrine spiradenoma is a benign tumor of the sweat glands. It was described in 1956 by Kersting and Helwig as an intradermal nodule, usually solitary, with paroxysmal pain crises. It occurs mostly in people aged 15 to 35, and most typically on the chest and face. 1-3 The tumor is usually covered by skin of normal or bluish color, and its typical location is the superficial or deep dermis, but can occasionally be found in the subcutaneous tissue. Although the face and chest are the most common sites, the tumor can occur in any body part. 1 It is a tumor with a long medical history and slow growth. 4 Malignization is rare but can take place. 5
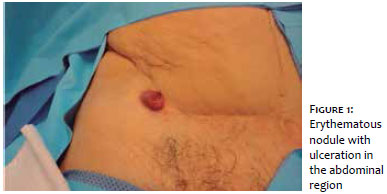
An 82-year-old female patient sought treatment for a lesion on the abdomen, around one year in development and with intermittent bleeding during the previous month. On examination, an erythematous, hardened nodule not adhered to the deep planes was found. (Figures 1 and 2)
The initial diagnostic hypotheses were sarcoma, amelanotic melanoma, B cell lymphoma, and cutaneous metastasis.
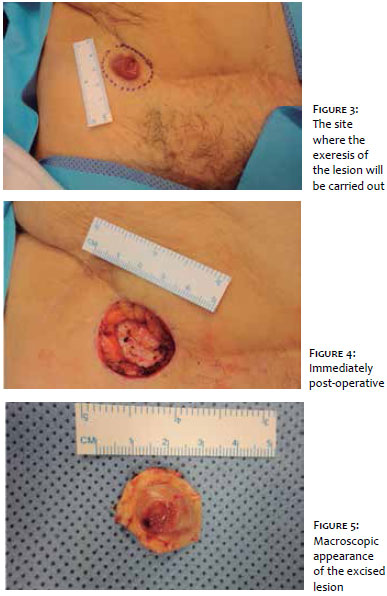
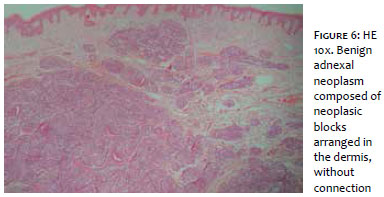
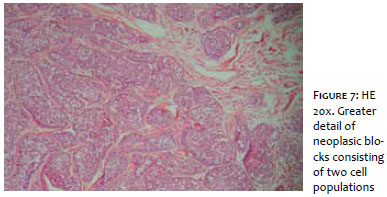
An incisional biopsy was performed, showing diffuse proliferation of monomorphic ovoid cells, sometimes with basaloid appearance, arranged in lobes septated by hyalinized bundles, and compatible with eccrine spiradenoma. The pathologist suggested the removal of the entire lesion (Figures 3 to 5), as well as new histology. The removal of the entire lesion was performed in a hospital setting by a plastic surgeon, with the new histology revealing a benign adnexal neoplasm composed of solid cell blocks arranged in the dermis, with no connection to the epidermis (Figure 6). The neoplastic blocks revealed small epithelial cells with a hyperchromatic nucleus and larger epithelial cells with pale cytoplasm around the luminal ductal structures (Figure 7).
The eccrine spiradenoma is an uncommon, benign tumor that arises from the sweat glandular apparatus and is one of nine painful skin tumors - the others being leiomyoma, neuroma, dermatofibroma, angiolipoma, neurilemmoma, endometrioma, glomus tumor, and granular cell tumor. 6
The tumor occurs either as solitary lesion (in 97% of cases and can reach a diameter of 5 cm) or as multiple lesions, which in some cases arise in linear or zosteriform distribution. 1, 6, 7 The lesions are typically small, well defined, and incorporated in normal sweat glands. 1
The precise etiology of the tumor is uncertain. The eccrine spiradenoma has never been observed in the glabra skin and arises as a benign adnexal neoplasm, with little or no differentiation, and historically assumed as originating from the eccrine lineage. However, it is known that the tumor often occurs along with other skin adnexal neoplasias such as: cylindroma, trichoepithelioma, and trichoblastoma - which favors the development of a follicle sebaceous-apocrine lineage rather than eccrine differentiation. Also, if the tumor was truly eccrine, it would be seen frequently on the palms or soles, rather than not at all, as in this case. 7
The main clinical feature is the presence of pain or sensitivity in about 91% of the patients, which usually occurs paroxysmally. It is believed that the pain is linked to small demyelinated axons that permeate the hyaline stromal mantle. In 1996, Crinton and Aravindan proposed that the pain could be related to the contraction of the tumor's myoepithelial cells, nevertheless electron microscopy has not proven the existence of these cells. Several studies have demonstrated the expression of the immunohistochemical marker S-100 in the tumor, suggesting the existence of a link with neural tissue, since S-100 protein is generally present in neural crest-derived cells, and chondrocytes, adipocytes, myoepithelial cells, macrophages, Langerhans cells, dendritic cells, and keratinocytes. Due to the presence of this protein in various cell lineages, it is not possible to precisely establish the relationship with the neural tissue. Nonetheless, a different study has demonstrated the presence of Langerhans cells with thin and irregular expansions dispersed among the tumor cells in the nodule. In a case study carried out by Park et al., 6 the sample was positive for S-100 only in the tumor's capsule, which was the exact position of disorganized, thickened nerve fibers. The authors of that study also confirmed the presence of a neural element with the positivity of an axon marker. 6 The differential diagnosis should include other causes of painful tumors but also: anaplastic carcinoma, adenocarcinoma, squamous and basal cell carcinomas, and other adnexal neoplasias, such as cylindromas; in addition to mesenchymal tumors. 1, 7
There can be a suspicion of malignant eccrine spiradenoma when there is the emergence of pain that did not previously exist, increased sensitivity, color change, rapid growth, or ulceration of a lesion that has remained stable for a long time. The suspicion of malignization should be thoroughly evaluated due to the aggressiveness of the malignant tumor, with a mortality rate that varies between 20% and 39%, and the lymph nodes, bones, lungs, and brain as main metastasis sites. 1, 4
Clinical suspicion is useful, however it is not sufficient to make the diagnosis. The definitive diagnosis will come from the histology of the skin biopsy. The cytology of a fine needle aspirate can also confirm the diagnosis. 7 In the histological examination, basophilic lobes are seen under smaller magnification due to the dense nuclei of tumor cells. Under greater magnification, basaloid cells comprising two distinct morphologies can be seen: in the first, the cells are larger, clearer, and with ovoid nuclei; in the second, the cells are smaller, darker, and with compact hyperchromatic nuclei. 5, 7
The treatment is essentially surgical, with the more common options being conventional surgery or the Mohs technique yielding small recurrence rates - and therefore the best treatment option aimed at preventing malignant transformation. 7
The present article reports the finding of a benign eccrine spiradenoma - a tumor of the sweat glands, with a poorly-defined etiology. The eccrine spiradenoma is a rare tumor that can emerge in various clinical forms. Its diagnosis is crucial due to the potential for malignant transformation of these lesions, especially in cases of multiple or symptomatic lesions. Malignant eccrine spiradenoma can be lethal if not diagnosed and treated, and a high index of suspicion is necessary in any benign lesion that rapidly changes its characteristics, i.e. consistent with a longstanding disease. Case reports, like the present, are important to maintain heightened suspicion regarding the diagnosis of this rare condition and in assisting in guiding an appropriate approach.
1. Yesilkaya Y, Demirbas B, Gokoz O, Akata D. Eccrine Spiradenoma of the Thigh: Sonographic findings and review of the literature. J Diagn Med Sonogr. 2012;28(6):311-313.
2. Hashimoto K, Gross BG, Nelson RG, Lever WF. Eccrine Spiradenoma: Histochemical and electron microscopic studies. J Invest Dermatol. 1966;46(4):347-65.
3. Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. 5 ed. Rio de Janeiro: Guanabara Koogan; 2008. p.554.
4. Berçin S, Kutluhan A, Metin A, Süren D. Malignant eccrine spiradenoma on the lateral margin of nose as an infrequent localization. Indian J Dermatol. 2009;54(2):173-175.
5. Storm CA, Seykora JT. Cutaneous Adnexal Neoplasms. Am J Clin Pathol. 2002;118(Suppl):S33-49.
6. Park HR, Im SB, Kim HK, Shin DS, Park YL. Painful Eccrine Spiradenoma Containing Nerve Fibers: A Case Report. Dermatology. 2012;224(4):301-6.
7. Englander L, Emer JJ, McClain D, Amin B, Turner RB. A Rare case of multiple segmental eccrine spiradenomas. J Clin Aesthet Dermatol. 2011;4(4):38-44.
This study was performed at a private practice - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}