


Alexandre Sabino Sisnando1; Luana Oliveira Ramos2; Fabio Francesconi3
Keywords: CARCINOMA, BASAL CELL; SURGERY, PLASTIC; SURGICAL FLAPS
The island flap has two basic characteristics: 1) the shape of the donor skin resembles an island that is detached from the surrounding epidermis and dermis on all sides; 2) a subcutaneous pedicle is maintained, thereby ensuring vascularization and allowing some mobility to the nearby receptor area. Variations of this type of flap depend on the shape of the island and the way it is transferred to the receptor area. Among these variations are: the traditional triangular island with V-Y advance, which can be single or double (bipedicled); the variant where the shape of the island and its size are similar to those of the defect and the transference is performed by transposition (the skin between the donor and receptor areas is excised) or interpolation (where a pedicle is left between the donor and the receptor area, with its subsequent removal during a second subsequent surgery); and the variant where the island, whose size and shape correspond to those of the surgical defect, is transferred through a tunnel created in the upper portion of the subcutaneous tissue. 1 The latter variant can be considered a type of interpolation, as the skin between the primary and secondary defects is not excised.
The present article describes two cases of basal cell carcinoma (BCC) in facial areas, each with difficult reconstruction, where the tunneled island flap technique was used, with an aim of demonstrating the application, characteristics, and possible complications of this method.
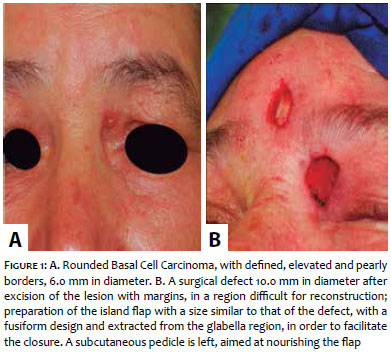
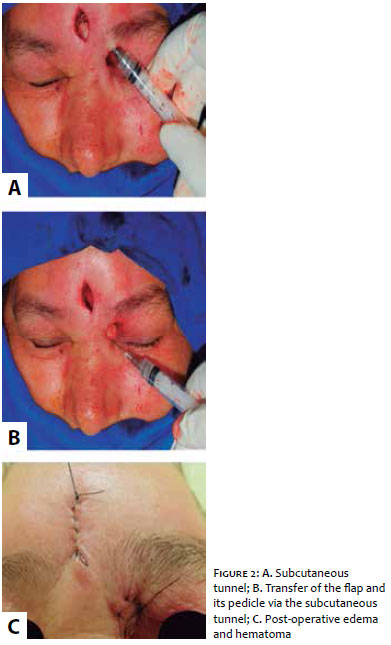
A 57-year-old woman presented with a round shaped basal cell carcinoma (BCC) with elevated and pearly borders in the medial corner of the upper left eyelid (Figure 1A). The patient underwent excision that resulted in a surgical defect 10 mm in diameter. An advancement flap would not be a good option in this case, as it would distort the anatomy of the region. A decision was made in favor of using a non-contiguous donor area (in the glabellar region). 2 For the preparation of the flap, a similar shape and size to those of the defect were implemented, however fusiform, aiming at facilitating the closure (Figure 1B). The dissection of the donor area was carried out, preserving a subcutaneous pedicle intended to nourish the flap. In the existing healthy skin between the primary and secondary surgical defects, a tunnel was created in the subcutaneous level using the blunt dissection technique (Figure 2A). Next, the island skin flap - together with the pedicle - was driven through the tunnel using a hook (which may be improvised with a small syringe and a 25x7 needle carefully bent at the tip, as in the present case) (Figure 2B).
Once positioned in the defect, the flap was sutured with 5.0 nylon thread and interrupted sutures. The post-operative period coursed with significant local edema, which is common in these cases and can be minimized with the application of cold compresses for 20 minutes, several times a day. There was no infection or necrosis (Figure 2C). The result was satisfactory, with no trapdoor effect, 3 nevertheless there was a slight bulging of the skin between the donor and the receiving areas (Figure 3). The post-operative histologic control of the surgical specimen revealed free margins.
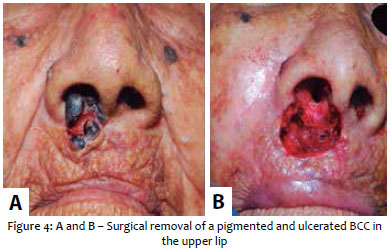
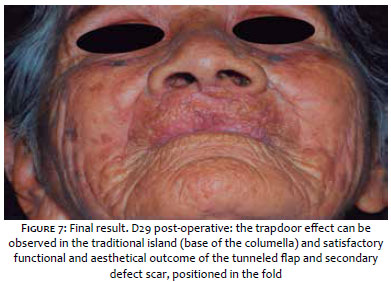
An 86-year-old female patient presented with a centrally ulcerated, pigmented BCC on the upper lip, advancing towards the right nostril, and measuring about 9 mm at its widest diameter. After excision with a 4.0 mm margin, a difficult to correct defect regarding the functional aspect was observed (Figure 4). A decision was made for a tunneled interpolation flap, in which the island's fusiform design in the nasolabial fold allowed for the suture of the secondary defect to be positioned in the fold, providing a good aesthetic appearance to the scar (Figure 5). In order to rebuild the base of the columella, a small island with traditional transposition was performed and tractionned with its pedicle into the defect using 5.0 nylon thread (also used in the suture), in a way that distributed the tension and facilitated the positioning of the tunneled flap (Figure 5). The post-operative period coursed uneventfully (Figure 6). The final result was functionally and aesthetically satisfactory, and the traditional trapdoor defect could be observed in the island 3 (in the columella's base), but not in the tunneled island (Figure 7).
BCC is the most prevalent skin cancer in humans. However, due to its low metastasizing capacity, it is usually curable with surgical exeresis in a single surgical procedure. 4
The tunneled island is a flap with a random pattern, whose blood supply depends on the vascular plexus of the deep dermis and subcutaneous. 5 It has the advantage of providing the surgical defect with a skin non-adjacent to the lesion but with the same characteristics of the surrounding area, thereby preserving the local anatomy. 6 The transference via a subcutaneous tunnel prevents the need for an incision in the skin between the donor and the receiving areas and allows the flap to be removed from a non-contiguous area 1, observing local characteristics and yielding a good cosmetic result. 7
In Case 1, the tunneled interpolation of the island avoided the distortion of the eyebrow region, as the primary defect was located on the upper eyelid. However, an undesirable effect of this flap is that at the moment of subcutaneous transfer, there is the addition of material beneath the skin, resulting in the elevation in the area through which the tunnel has been created. 1 This took place in the first case described. Had the lesion been located in the nasociliary region, 2 a traditional transposition of the island would have been be the best option, producing however, a secondary defect in the glabellar region. 8
In Case 2, due to the fact that the lesion was located on the upper lip, the reconstruction was aimed at preserving the anatomy, owing to the aspects of the functional and aesthetic appearance, requiring extra attention in regards to the positioning of the vermilion and the transition line between the skin and the semimucosa, preserving the lip contour, the position of the philtrum, and the bilateral symmetry regarding the nasolabial folds. 9 Among the various techniques available for the reconstruction of this region, the island flap has been shown to be a good option for it causes little distortion of the anatomy and low scar retraction, and also offers ease in positioning the suture of the secondary defect in the nasolabial fold, yielding a good cosmetic result.
The island flap with subcutaneous tunnel interpolation is a very useful resource in the surgical repair of certain surgical defects following the exeresis of a carcinoma in the face, especially when it is possible to achieve a cosmetically acceptable secondary defect scar - in a natural fold of the skin or in an area where the appearance of rhytids is common - and when seeking consistency between the flap and the skin around the primary defect.
1. Kimyai-Asadi A, Goldberg LH. Island pedicle flap. Dermatol Clin. 2005;23:113-27.
2. Tamura BM. Topografia facial das áreas de injeção de preenchedores e seus riscos. Surg Cosmet Dermatol. 2013;5(3):234-8.
3. Li JH, Xing X, Liu HY, Li P, Xu J. Subcutaneous Island Pedicle Flap - Variations and Versatility for Facial Reconstruction. Ann Plast Surg. 2006;57(3):255-9.
4. Morselli P, Zollino I, Pinto V, Brunelli G, Carinci F. Evaluation of clinical prognostic factors in T1 N0 M0 head and neck basal cell carcinoma. J Craniofac Surg. 2009;20(1):98-100.
5. Wang SQ, Goldberg LH, Kimyai-Asadi A. Tunneled Island Pedicle Flap for an Earlobe Defect. Dermatol Surg. 2007;33(7):835-7.
6. Mahlberg MJ. Tunneled Melolabial Pedicle Flap for Small but Deep Lateral Alar Rim Defect. Dermatol Surg. 2013;39(10):1527-9.
7. Pontello Júnior R, Kondo RN, Pontello R. A utilização do retalho A-T para reconstrução de ferida operatória no dorso da mão. Surg Cosmet Dermatol. 2013;5(3):270-2.
8. Campbell LB, Ramsey ML. Transposition island pedicle flaps in the reconstruction of nasal and perinasal defects. J Am Acad Dermatol. 2008;58(3):434-6.
9. Lopes Filho LL, Lopes LRS, Villa Neto AB, Costa TS. Carcinoma basocelular no lábio superior: tratamento cirúrgico e reconstrução com retalho de transposição. Surg Cosmet Dermatol. 2011;3(3):243-5.
This study was performed with patients operated on at the Fundação Centro de Controle de Oncologia do Estado do Amazonas (FCECON), an associate hospital for supporting the medical residency services of the Fundação de Medicina Tropical Heitor Vieira Dourado (FMT-HVD) and of the Hospital Getúlio Vargas (HUGV) - Manaus (AM), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}