


Jeane Jeong Hoon Yang1; Antônio José Tebcherani2; Ed Wilson Tsuneo Rossoe3
Keywords: NEOPLASMS, ADNEXAL AND SKIN APPENDAGE; SYRINGOMA; ADENOMA, PLEOMORPHIC
Chondroid syringoma, also known as cutaneous mixed skin tumor, is a rare tumor of the skin appendages, and consists of epithelial and mesenchymal elements. The presence of sweat glands surrounded by cartilage matrix, led to the name chondroid syringoma. 1 It can clinically resemble different skin lesions, for it does not present particular clinical features. 2 Among the differential diagnoses are basal cell carcinoma, pilomatricoma, steatocystoma; therefore histological examination is required for diagnostic confirmation. 3 We report the case of a rare clinical presentation of a chondroid syringoma simulating a basal cell carcinoma.
A 71-year-old Caucasian male patient described the appearance of a lesion on the left brow five years earlier, gradually increasing in size during the last two years, but asymptomatic. The patient was a former alcoholic (in recovery for 10 years). A dermatological examination showed a pearlescent/pearly colored nodule with telangiectasias on the surface, measuring around 1.5 cm (Figure 1). A diagnostic hypotheses of a basal cell carcinoma, pilomatricoma, sebaceous cyst was formulated and a decision was made for the surgical removal of the lesion. The patient is receiving outpatient treatment, with good clinical improvement.
Chondroid syringoma is a rare, benign adnexal skin tumor, originally described in 1859 by Billroth as a mixed skin tumor due to the existence of both epithelial and stromal components. The presentation of sweat gland components defined in cartilaginous stroma led Hirsch and Helwig to name this lesion chondroid syringoma in 1961. 1 These authors proposed five histologic criteria for its diagnosis: 1) nests of cubic or polygonal cells; 2) intercommunicating tubular alveolar structures flanked by two or more rows of cubic cells; 3) ductal structures consisting of one or two rows of cubic cells; 4) occasional cysts with keratin; 5) a variable composition matrix. 1 It is clinically characterized by a single nodule with a smooth surface, non-adherent to the deep planes and with precise limits, asymptomatic, located mainly on the face or neck, and most commonly on the nose, lips, and eyebrows, as in the present case. Less commonly, it may involve hands, feet, axillae, abdomen, penis, scrotum, and vulva. 4 It grows slowly and progressively. Its size typically varies between 0.5 and 3.0 cm 5 (the studied patient had lesions of 1.5 cm in diameter). It is usually found in men (mean age around 50 years), with a gender ratio ranging from 1.3/1 and 5/1.3 There is an absence of any particular clinical feature, and the diagnosis is essentially histological. 4 There is a presence of epithelial components (glandular structures with eccrine or apocrine differentiation, or both) and mesenchymal components (tissue with myxoid, chondroid, adipose or fibrous tissue differentiation). The epithelial component comprises glands that can be histologically of two types: the apocrine (as in the present case - the most common type, constituted by focally connected tubular or cystic glands, fringes with a double seat of cubic or flattened cells); and the eccrine (characterized by a narrow lumen and glands framed by a single layer of cells). Although the immunohistochemical study is dispensable for the diagnosis due to the lesion's dual population feature (glandular structures and cartilaginous components), there are studies reporting the expression of cytokeratin (CK), epithelial membrane antigen (EMA), carcinoembryonic antigen (CEA) in the glandular structures, vimentin, S-100 protein, neuronspecific enolase (NSE), and in some cases glial fibrillary acidic protein (GFAP) in the cartilaginous component. 6
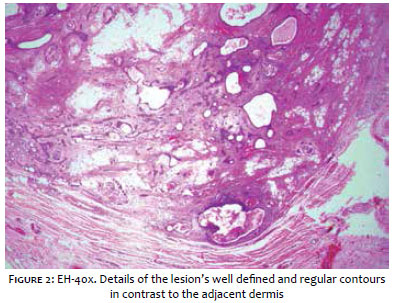
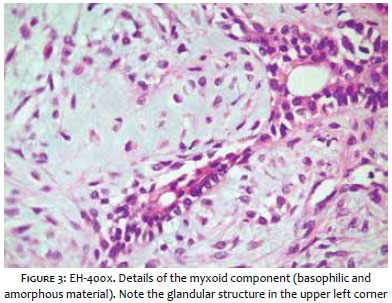
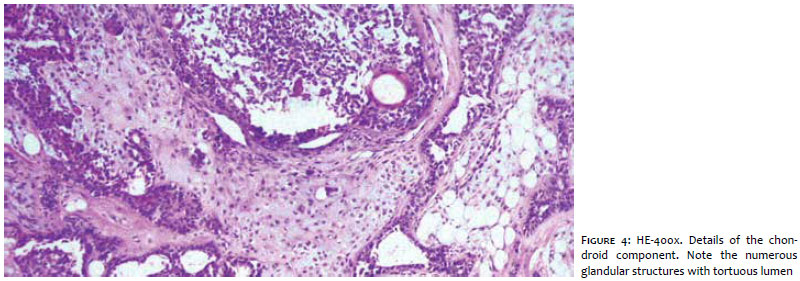
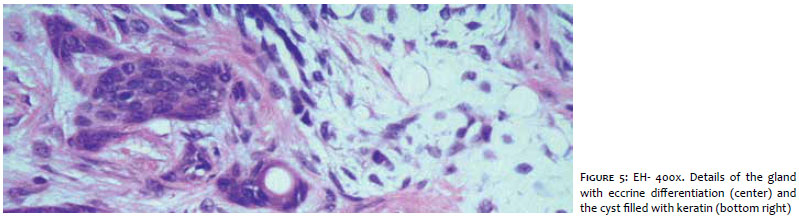
The case reported has considerably exuberant epithelial and mesenchymal components, in addition to the important fact that the lesion's limits are well defined (Figure 2). This, together with the absence of atypias, favors its benign nature. The mesenchymal component has myxoid (Figure 3) and chondroid (Figure 4) elements, in addition to foci of adipose differentiation. The glandular part of the tumor is sometimes constituted by glands with regular and reduced lumen (which resemble the secretory portion of eccrine sweat glands) (Figure 5), and sometimes by glands with ectatic and tortuous lumen, suggestive of apocrine differentiation. Cysts filled with keratin are also present (Figure 5). The chondroid syringoma has no specific clinical characteristics and resembles other skin lesions. Among the differential diagnosis it is possible to mention epidermal inclusion cysts, amelanotic nevi, sebaceous cysts, dermoid cysts, schwannomas, neurofibromas, pilomatrixomas and basal cell carcinomas. 7 In the present case, the patient had clinical features resembling those of a basal cell carcinoma. Most cases are benign, although there are rare malignant forms. 1,2 Malignant types most commonly occur in young women and often measure more than 3.0 cm, are locally invasive and show a predilection for the trunk or extremities. 1,2 Histological features considered to be signs of malignant transformation are: cytologic atypia, infiltrative margins, satellite tumor nodules, tumor necrosis, and the involvement of deep structures, 8 - which were not seen in the present case. The treatment of choice is excision with the removal of 4.0 mm of normal peritumoral tissue. Surgery is often straightforward due to the good delimitation of the lesion by a capsule. In the present case, the lesion was excised entirely. There was no recurrence during the initial three months of follow-up. The patient remains under observation. Other treatment options described are dermabrasion, electrodessication, and vaporization with Argon or CO2 laser. 4 Incompletely resected benign tumors require periodic monitoring aimed at detecting possible recurrence or malignant transformation. 7
1. Hirsch P, Helwig EB. Chondroid syringoma. Mixed tumor of skin, salivary gland type. Arch Dermatol. 1961;84:835-47.
2. Solanki LS, Dhingra M, Bhalla M, Thami GP, Punia RPS, Shilpy Batra S. Chondroid syringoma: Report of two cases in young patients. Dermatol Online J. 2011;17(12):7.
3. Abila S, Bouhllaba J, Zarkika S, Lamchahaba FZ, Saidib A, Ismailia N, et al. Syringome chondroïde de la face. Ann Dermatol Venereol. 2012;139(10):681-3.
4. Yavuzer R, Basterzi Y, Sari A, Bir F, Sezer C. Chondroid syringoma: a diagnosis more frequent than expected. Dermatol Surg. 2003;29(2):179-81.
5. Tokyol C, Aktepe F, Yavas BD, Yildiz H, Aycicek A. Chondroid syringoma: a case report. Acta Cytol. 2010;54(8):973-6.
6. Argenyi ZB, Balogh K, Goeken JA. Immunohistochemical characterization of chondroid syringomas. Am J Clin Pathol. 1988;90(6):662-9.
7. Varsori M, Dettwiler S, Chaloupka K. Syringome chondroïde de la paupière: à propos d'un cas. J Fr Ophtalmol. 2007;30(1):3.
8. Bates AW, Baithun SI. Atypical Mixed Tumor of the Skin: histologic, immunohistochemical, and ultrastructural features in three cases and a review of the criteria for malignancy. Am J of Dermatopathol. 1998;20(1):35-40.
This study was performed at Complexo Hospitalar Padre Bento de Guarulhos (CHPBG) - Guarulhos (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}