


Luciana Martins Rodrigues Salgado1; Livia de Vasconcelos Nasser Caetano2; Gabriela Moura de Paula3; Maria Auxiliadora de Paula Carneiro Cysneiros4; Luiz Fernando Fróes Fleury Junior5
Cutaneous leiomyosarcoma is a rare neoplasm with a tendency to recur, and with possible metastases. The authors report a case of a female patient who was being treated with triamcinolone injections in a dermal leiomyosarcoma lesion that was misdiagnosed as keloid.
Keywords: KELOID; LEIOMYOSARCOMA; SKIN NEOPLASMS
Cutaneous leiomyosarcoma (LMS) is a rare neoplasia corresponding to 2-3% of soft tissue sarcomas. 1 It is likely derived from piloerector smooth muscle (dermal LMS) or from smooth muscle of the vascular wall in the subcutaneous (subcutaneous LMS), 1-6 with a different biological behavior. It is prevalent in Caucasian men in their 5th and 6th decades of life. 2
Its subcutaneous form consists of a bulging covered with normal and mobile skin over the lesion. Recurrence is high (up to 70%) and there is a risk of metastases.1
Primary cutaneous LMS (dermal) has a relatively indolent behavior. The recurrence rate is around 30%, 5 but can be absent in some series. 2 Its extension up to the subcutaneous level brings a higher risk of recurrence, 1 though the risk of metastasis is low2-4 and even controversial.3, 5 It comes in the form of a single tumor of up to 3 cm,2, 6 well-defined, lobulated, pedunculated or umbilicated and varying in color (erythematous to brownish).5 When grouped in nodules, the presence of an extracutaneous primary neoplasm should be investigated, especially in its retroperitoneal or uterine forms.1 There may be pain on compression, as well as exulceration and bleeding.1, 5 It mainly affects areas in the thighs having a high hair density, as well as the head and neck.1-2, 6
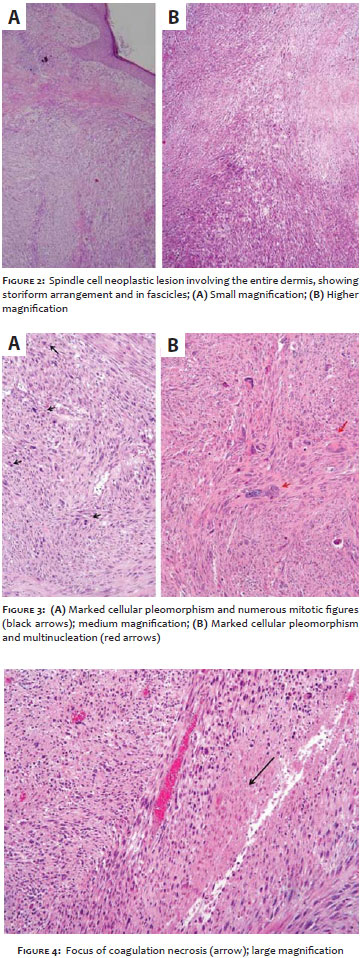
Histology shows a smooth muscle cell tumor, with proliferation of fusiform cells with elongated,"cigar-shaped" nuclei, pleomorphism, and mitosis. Immunohistochemistry identifies the smooth muscle cells, with smooth muscle actin, desmin, and vimentin as its main markers.1-6
The authors describe a case of leiomyosarcoma in which, due to the rarity of the condition, there had been a delay in the treatment due to lack of previous clinical suspicion.
A 49-year-old female patient was referred by a plastic surgeon for a differential diagnosis evaluation of a keloid lesion, after unusual response to corticosteroid injection.
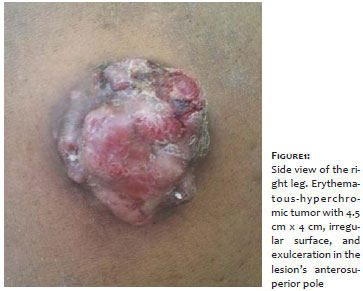
There had been an onset of a painful lesion with keloidal appearance on the lateral side of the right leg, six years earlier. The patient underwent excision with three recurrence episodes of the lesion, the last of which was three years before the submission of the present paper. She reported previous histologies with no malignancy, however the results were not in her possession. After eight monthly sessions of local injections of triamcinolone, she developed erythema, a worsening of pain, and changes in the lesion's appearance. Clinical examination showed an erythematous tumor of 4.5 cm x 4 cm, having an irregular surface and exulceration in the anteroposterior pole (Figure 1). The incisional biopsy revealed a clearly differentiated spindle cell neoplasm (Figure 2-4) with positive immunohistochemistry for smooth muscle actin, desmin, and S-100, and weakly positive for AE1/AE3. The diagnosis was consistent with leiomyosarcoma. Laboratory tests for the detection of a possible primary focus of neoplasia came back negative.
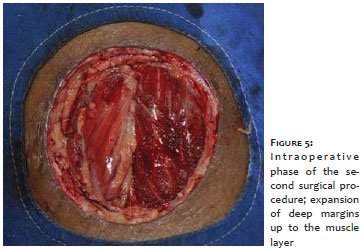
The resection of the lesion was performed with a 1 cm margin and a dissection depth up to the muscle fascia. A decision was made for the purse string suture with the aim at hemostasis and the plan for a later reconstruction. After the histological examination evidenced an excessively narrow deep margin, the dissection was extended up to the muscle layer (Figure 5). A total skin graft was performed in the third surgical stage. The patient progressed without complications or signs of recurrence during the observation period (eight months) and remains under clinical follow up (Figure 6).
The cutaneous leiomyosarcoma is a rare neoplasm and arises as a tumor that varies in color, shape, and size, and is more common in men.1-6 In the case described, the patient is female, phototype IV, and the disease emerged with a topography that was diverse from the usual.
Due to its nonspecific clinical features, diagnosis of leiomyosarcoma depends on the histologic examination and immunohistochemistry. In the present case, the patient had started treatment motivated by a clinical suspicion of keloid. However, she did not have a typical lesion and therefore her case deserved further investigation, given that various tumors and even infectious diseases may have a keloidal aspect.
The benefit of imaging examinations for pre-operative/diagnostic staging is not clear, and results are often negative.2 Although there is no clear guidance in the literature, a decision was made in this case to research and rule out other neoplasms (retroperitoneal, uterine) or metastases (lymph node, lung).
The lesion exeresis is the treatment of choice, with safety margins being suggested at 1 cm2 or the use of Mohs micrographic surgery (MMS).4 Adjuvant radiation therapy is mentioned, especially for lesions in excess of 5 cm, deep or where it is impossible to widen margins.2 The main prognostic factor is the status of the surgical margins,2-3 in addition to the size of the tumor,1 extension of the subcutaneous involvement1, 6 and mitotic index.1
In the present case, the surgery depth was increased, since the deep, free margin was deemed excessively narrow. A decision was made for not closing the surgical wound during the first operative time and to wait for confirmation from pathology that the removal of the lesion was complete, before the implementation of the graft. This technique is also described by other authors for the treatment of leiomyosarcomas and other tumors. 2
The patient's elapsed follow up time after the surgery is still short, however she remains under monitoring. The literature does not specify whether there is a necessary and limited follow up time or whether it should be continued, as is the case in the authors' dermatological service.
The present case exemplifies the importance of considering the differential diagnosis in dermatology. Although the clinical aspect is sufficient in a great number of cases, the histology is crucial for the identification of rare dermatoses that demand different therapeutic approaches. When considering lesions of a keloidal aspect, the absence of previous trauma, a positive personal and family history and the presence of pain should trigger an alert.
1. Holst VA, Junkins-Hopkins JM, Elenitsas R. Cutaneous smooth muscle neoplasms: clinical features, histologic findings, and treatment options. J Am Acad Dermatol. 2002;46(4):477-90.
2. Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20(4):307-12.
3. Hall BJ, Grossmann AH, Webber NP, Ward RA, Tripp SR, Rosenthal HG, et. al. Atypical intradermal smooth muscle neoplasms (formerly cutaneous leiomyosarcomas): case series, immunohistochemical profile and review of the literature. Appl Immunohistochem Mol Morphol. 2013;21(2):132-8.
4. Starling J 3rd, Coldiron BM. Mohs micrographic surgery for the treatment of cutaneous leiomyosarcoma. J Am Acad Dermatol. 2011;64(6):1119-22.
5. Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81(3):207-21.
6. Winchester D, Hocker TL, Brewer JD, Baum CL, Hochwalt PC, Arpey CJ, et al. Leiomyosarcoma of the skin: Clinical, histopathologic, and prognostic factors that influence outcomes. J Am Acad Dermatol. 2014;71(5):919-25
This study was carried out at the Universidade Federal de Goiás (UFG) - Goiânia (GO), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}