


Carlos Augusto Zanardini Pereira1; Luiz Carlos Pereira2; Ivo Acir Chermicoski3; Margarete Iassuko Furusho4; Valéria Zanela Franzon4,5
Since ancient times, humans have had an interest in improving their body contour. Liquid silicone has been used for this purpose, in order to improve deformities. The authors present a case of a female patient with paralysis in the right lower limb, who underwent improper injections of a large volume of injectable silicone in the affected limb aimed at correcting its contour. Ten years later, the patient developed local complications linked to the silicone injections - localized scleroderma lesions and superficial lipomatous nevus with progressive growth in the affected limb - and clinical and laboratory pictures of rheumatoid arthritis. Injectable liquid silicone should be contraindicated as a substance for implants.
Keywords: POSTOPERATIVE COMPLICATIONS; SILICONES; SKIN NEOPLASMS
Between 1960 and 1970, physicians and lay people worldwide used silicone oil injections or industrial silicone to enlarge breast size and improve the body's contour. After a variable period ranging from three to twenty years, many of the individuals who received such injections developed serious complications, ranging from product migration causing siliconoma (foreign body reaction), auto-inflammatory disease, and even carcinomas, leading to the cessation of this technique and its prohibition by the Food and Drug Administration (USA) and the Dimed in Brazil. 1
In a retrospective study carried out from 1960 to 1996 with more than seven thousand patients who underwent silicone breast implantation, it was possible to observe the presence of a probable risk of rheumatoid arthritis, lupus erythematosus, scleroderma or Sjögren's syndrome development. 2
The superficial cutaneous lipomatous nevus is an idiopathic abnormality, being considered a variant of the connective tissue nevus. It is histologically characterized by the presence of ectopic mature adipose tissue in the dermis. The rarest is the Hoffmann-Zurhelle variant, which consists of nodular or "mamillated" lesions grouped in cerebriform plaques in a segmental arrangement. It is usually congenital or emerges in the first three decades of life, having the pelvis and buttocks as its primary location.3
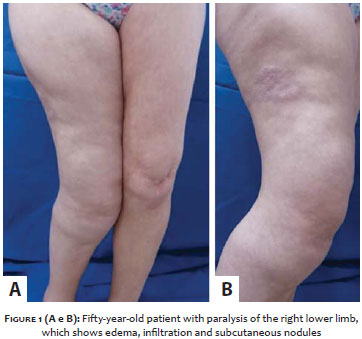
The present study describes the case of a 50-year-old Caucasian married female patient, with polio sequelae in the right leg. She described having undergone a large volume implant of injectable silicone in the affected limb in procedures performed by physicians in 1994, aimed at improving the contour of the thigh and leg, which had been disfigured by the polio sequelae (Figure 1).
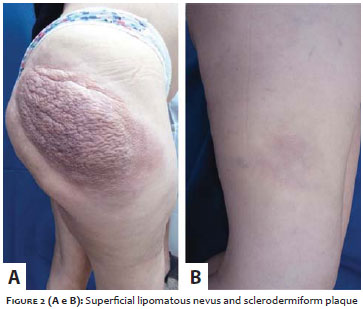
Approximately 10 years after the procedure had been carried out, the patient attended her first medical visit at the Fundação Pró-Hansen, describing cutaneous complications consisting of hardening of the skin of the right lower limb, with formation of asymptomatic erythematous plaques - possibly characterizing the clinical picture of morphea - and of a verrucous erythematous-pigmented plaque of approximately 15 cm x 25 cm and with progressive growth in the right gluteal region, which led to the suspected diagnosis of lipomatous nevus (Figure 2). The clinical and laboratory diagnosis of rheumatoid arthritis was also made at the time. According to the patient's report, there was no family history of the condition.
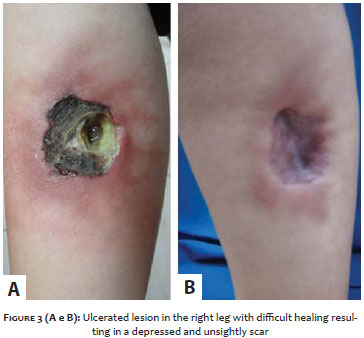
In 2011, the patient sought care at the Fundação Pró-Hansen presenting a poorly healing ulcer on the right leg following a trauma on the hardened plaque. The wound's debridement and cleansing were carried out, with the daily change of dressings with healing ointment and the administration of systemic antibiotics. Complete re-epithelialization occurred after four months of treatment, resulting in a depressed and unsightly scar (Figure 3). Laboratory tests, incisional biopsies of the hardened plaque and the verrucous lesion, as well as a MRI of the affected limb were carried out. The rheumatoid arthritis continued to be treated with 7.5 mg/week methotrexate and 1g/day paracetamol.
Histology
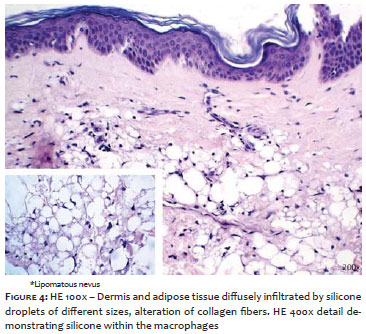
Hardened plaques: dermis and adipose tissue diffusely infiltrated by silicone droplets of different sizes, in addition to the presence of silicone within the macrophages and alteration of collagen fibers (Figure 4).
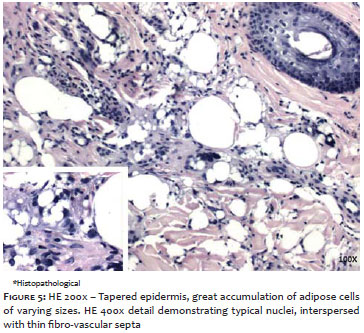
Verrucous lesion: tapered epidermis, with great accumulation of adipose cells of varying sizes, compatible with histological diagnosis of superficial lipomatous nevus (Figure 5).
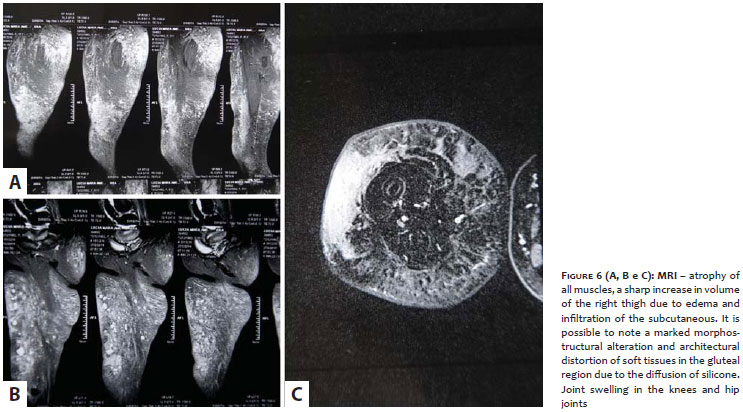
MRI: atrophy of all muscles, sharp increase in volume of the right thigh due to edema and infiltration of the subcutaneous. It was possible to observe a marked morphostructural alteration and architectural distortion of the soft tissues in the gluteal region due to the diffusion of silicone (siliconoma). Presence of joint effusion in the knee and hip joints (Figure 6).
Laboratory tests: FAN (-), AntiRO (-), AntiLA (-), ESR 50mm/h, rheumatoid factor (+) 60UI/ml, blood count (normal) and liver function tests (normal).
Almeida Jr, Gevehr and Pinto4 reported a case of late onset of superficial lipomatous nevus, which is the only publication to date featuring this content. The pathogenesis in superficial lipomatous nevus is not well understood. Some authors suggest that this lesion originates from adipose precursor cells, as they were observed in the vicinity of the nevi, however this fact was not confirmed by electron microscopy.
The patient whose case is described in the present case report also referred to the late onset of the lesion, after 40 years of age.
Brotas et al. 5 reported a case of a 40-year-old female patient who presented coalescing erythematous papules, forming a scleroderma plaque throughout the gluteal region two years after the application of liquid injectable silicone in the region.
A syndrome called ASIA (Autoimmune/Autoinflammatory Syndrome Induced by Adjuvants) has recently been incorporated into the "siliconoses", a term referring to the various events that occur after exposure to silicone. This syndrome's pathogenesis is based on the hypothesis that early exposure to an adjuvant can trigger a chain of biological and immunological events, which in susceptible individuals, can lead to the development of autoimmune diseases. The hypothesis that allowed linking breast implants with the development of autoantibodies was that of the presence of an adjuvant action.6
The silicone can migrate from the site of application to nearby or even distant body sites, with the presence of granulomas in the anterior and posterior sides of the lower limbs - resulting from the application of substances for increasing the thighs and buttocks - becoming increasingly common. The cause for the product's migration is the large volume applied at short intervals, a fact that allows the silicone to travel to distant sites through the tissular planes.7
In an article published by Silva,8 a patient received injectable industrial liquid silicone in the breast, with complications ten years later. The patient developed abscesses that led to a bilateral mastectomy 35 years later, due to complications caused by the siliconoma.
In addition, there was a report of a case of a woman who underwent the application of injectable liquid silicone in both buttocks, with a late onset of difficult to resolve ulcerations. 9
In the present case report, the ulcer that wouldn't heal was located on a hardened plaque, and infiltrated with silicone, according to the pathological examination.
Shvartsbeyn et al.10 published a case of a 35-year-old transsexual woman with bilateral masses in the buttocks, in which the histopathological evaluation revealed a collection of cells with cytoplasmic vacuoles containing lipids similar to lipoblasts. This pattern can be clinically and histologically mistaken for neoplastic processes, particularly when this adverse effect of the industrial silicone develops several years after injection.
Among the environmental factors that compromise the immune system are the adjuvants (silicone, aluminum, pristine and infections, among others), which can be deemed as being the "triggers" that initiate autoinflammatory diseases in humans.6-11
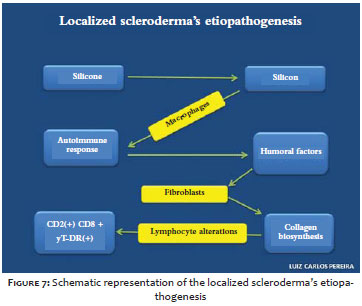
The etiopathogenesis of localized scleroderma (morphea) can be explained by the presence of silicone in the body turning into silica or silicon, and producing an autoimmune response with macrophages that phagocytoses silicon and releases humoral factors. The latter, in turn, trigger the biosynthesis of collagen by fibroblasts that induce lymphocyte alterations in the subpopulations CD2 +, CD8 + y T-DR (+) 11 (Figure 7).
The literature has not reported to date any case of patients with poliomyelitis sequelae who have undergone implants with injectable silicone, for the purpose of trying to improve the body's aesthetic and coursing with serious late onset complications arising from such conduct. Liquid injectable silicone should be contraindicated as a material for implantation. It is a drug that brings late onset complications when injected directly into human tissue and can cause local and systemic complications, interfering with the immune system and causing the development of autoimmune diseases. Deformities and damage to the healing of cutaneous wounds can take place due to the migration of the liquid. The etiology of lipomatous nevus remains unclear. Further studies are needed due to its rarity, especially regarding their possible correlation with liquid silicone implant.
We would like to thank Dr. Maurizio Pedrazzani from X-Leme diagnostic imaging; Dr. Lismari A.F. Mesquita, Dermatopathologist Physician at the Dermatology Service of the Santa Casa de Curitiba; Dr. Samuel Regis de Araújo, Pathologist Physician at Laboratório Master pathology and cytopathology.
1. Freitas RJ, Cammarosano MA, Rossi RHP, Bozola AR. Injeção ilícita de silicone líquido: revisão de literatura a propósito de dois casos de necrose de mamas. Rev Soc Bras Cir Plast. 2008;23(1):53-7.
2. Brinton LA, Buckley LM, Dyorkina O, Lubin JH, Colton T, Murray MC, et al. Risk of Connective Tissue Disorders among Breast Implant Patients. Am J Epidemiol. 2004;160(7):619-27.
3. Morales AL, Zaballos PR, Concepción G, Matilde P, Carapeto FJ. Nevus lipomatoso cutáneo superficial (Hoffman-Zurhelle) / Nevus lipomatosus cutaneous superficialis (Hoffman-Zurhelle). Med Cután Ibero Lat Am. 2003;31(4): 233-7.
4. Almeida Jr HL, Gevehr D, Pinto IO. Nevo lipomatoso superficial de aparecimento tardio. An Bras Dermatol. 1999;74(6):601-3.
5. Brotas AM, Sousa TJE, Silva GCS, Motta ALSPG, Coelho ABA. Pseudovesiculação infiltração e esclerose cutânea: exuberância clínica do granuloma por silicone. RBM- Rev Bras Med. 2014;71(6):5-8.
6. Shoenfeld Y, Agmon-Levin N. ‘ASIA’ - Autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmun. 2011;36(1):4-8.
7. Altmeyer MD, Anderson LL, Wang AR. Silicone Migration and granuloma formation. J Cosmet Dermatol. 2009;8(2):92-7.
8. Silva RF, Rios LR, Carvalho Garbi Novaes MR, Silva EL. Evolução de 45 anos de siliconoma de mama. Relato de caso. Com Ciências Saúde. 2011;22(3):271-6.
9. Herink C, Zwaka PA, Schön MP, Mempel M, Seitz CS. Serious complications following gluteal injection of silicone. Hautarzt. 2013;64(8):599-602. doi: 10.1007/s00105-013-2573-6. German
10. Shvartsbeyn M, Rapkiewicz A. Silicon-associated subcutaneous lesion presenting as a mass: a confounding histopathologic correlation. Hum Pathol. 2011;42(9):1364-7.
11. Panzarelli A, Gonçalves JC. Esclerodermia localizada (morfea) posterior a implante mamario. Dermatol Venez. 2012;50(2):50-3.
This study was carried out at the Pró-Hansen Foundation - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}